
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
The Neuroscience of Marijuana
The neuroscience of cannabis has advanced at a remarkable pace. While it’s a complicated story, the basic effects of marijuana on our brains are pretty well established and fairly easy to grasp. Some knowledge of these effects can be clinically useful, particularly when it comes to predicting the potential effects of excessive THC that your patients may ingest.
To set the scene, recall the big picture: Our brains are composed of billions of neurons that communicate signals to one another via neurotransmitters (NTs) and whose activity is further mediated by numerous neuroregulators (NRs). There are dozens of types of NTs—some are widely distributed throughout the brain, such as glutamate and GABA, while others work in smaller and more specific brain areas. These include serotonin, dopamine, and norepinephrine—NTs that we manipulate with many of our psychiatric drugs.
What you probably didn’t learn during your training is that one of the most extensive neuroregulatory systems in the human brain (or in any animal brain, for that matter) is the endocannabinoid system (ECS). The ECS is an ancient NR system, and contrary to the strong belief of many adolescents and adults, its primary function is not to allow people to get high from smoking joints. Rather, it serves as one of the major neural modulators of the nervous system.
Here’s how the ECS works. When a typical neuron is activated, it releases NTs into the synaptic cleft. The NTs travel across this tiny gap to bind to a specific receptor on the other side of the synapse. The binding then causes a chemical and electrical process that depolarizes the next neuron, creating an action potential that then activates the next neuron, and so on in a domino effect. This is how garden-variety NTs like glutamate and dopamine work.
But neurons need a modulating mechanism—something to put the brakes on neurotransmission so that our brain machinery can be finely tuned. That’s the job of our endogenous cannabinoids, known as endocannabinoids. There are two of them: anandamide (named from the Sanskrit word for bliss) and 2-arachidonoyl glycerol.
The building blocks of the endocannabinoids are stored within the postsynaptic neurons. When an NT activates the postsynaptic neuron, it starts a process that synthesizes endocannabinoids and spits them out into the synaptic space. These endocannabinoids then travel backwards, or upstream, to the presynaptic neuron, where specialized cannabinoid receptors are located. (There are two cannabinoid receptors, called CB1 and CB2. The CB1 receptors live mainly in the brain, while the CB2 receptors are in the immune system.) Once the endocannabinoids bind to the cannabinoid receptors, they act to inhibit the neuron from firing. The process is known as “retrograde transmission” and causes “presynaptic inhibition”—ie, reduced NT release.
In other words, a primary function of the ECS is to buffer the brain’s NT activity. This buffering process affects both excitatory (mainly glutamatergic) and inhibitory (mainly GABAergic) circuits. Putting the brakes on a glutamate neuron slows things down. But inhibiting a GABA neuron means reducing inhibition, so it speeds things up. Some researchers think that this dual effect helps to explain the various paradoxical psychoactive effects of cannabis: For example, the drug causes drowsiness on the one hand but enhances sensory experience on the other; it decreases anxiety at low doses but worsens it at higher doses.
This brings us right into the next topic—how does THC affect the ECS?
THC’s effect on the ECS
When someone uses marijuana, THC insinuates itself throughout the user’s ECS, latching onto cannabinoid receptors all over the brain and crowding out endocannabinoids. What does this mean for perception, emotion, and behavior? That depends on which parts of the brain we’re talking about.
This figure shows brain structures that are loaded with cannabinoid receptors and therefore especially vulnerable to the effects of THC. The psychoactive effects of THC match up pretty neatly with specific brain structures. For example, pot’s impairment of short-term memory is likely due to THC slowing down neurotransmission in the hippocampus, where we normally create memories. Its usefulness for chronic pain may be an effect of influencing transmission in the spinal cord.
An interesting side note (one that should make all stoners happy) is that there are no cannabinoid receptors in the brain stem, which is responsible for respiration. This means high doses of pot do not cause respiratory depression and death—unlike opioid overdoses.
The bottom line for your patients
How can you use your knowledge of the ECS in your interactions with teenage pot smokers? Tell patients that we now know a lot about how pot works in specific areas of the brain. They will be fascinated that the brain makes its own cannabinoids to keep itself functioning smoothly. However, non-endogenous cannabinoids, such as THC, throw this system off kilter. If this happens occasionally, little if any harm is done. However, constant use—or perhaps use at critical periods of brain development, such as early adolescence—is apt to spark long-term effects such as poorer motivation and difficulty learning and remembering information.
Will sharing this simplified version of marijuana neuroscience have an impact on your patients? You won’t know unless you try. (For more information, see Journal of Psychoactive Drugs January–March 2016;48(1).)
Child PsychiatryTo set the scene, recall the big picture: Our brains are composed of billions of neurons that communicate signals to one another via neurotransmitters (NTs) and whose activity is further mediated by numerous neuroregulators (NRs). There are dozens of types of NTs—some are widely distributed throughout the brain, such as glutamate and GABA, while others work in smaller and more specific brain areas. These include serotonin, dopamine, and norepinephrine—NTs that we manipulate with many of our psychiatric drugs.
What you probably didn’t learn during your training is that one of the most extensive neuroregulatory systems in the human brain (or in any animal brain, for that matter) is the endocannabinoid system (ECS). The ECS is an ancient NR system, and contrary to the strong belief of many adolescents and adults, its primary function is not to allow people to get high from smoking joints. Rather, it serves as one of the major neural modulators of the nervous system.
Here’s how the ECS works. When a typical neuron is activated, it releases NTs into the synaptic cleft. The NTs travel across this tiny gap to bind to a specific receptor on the other side of the synapse. The binding then causes a chemical and electrical process that depolarizes the next neuron, creating an action potential that then activates the next neuron, and so on in a domino effect. This is how garden-variety NTs like glutamate and dopamine work.
But neurons need a modulating mechanism—something to put the brakes on neurotransmission so that our brain machinery can be finely tuned. That’s the job of our endogenous cannabinoids, known as endocannabinoids. There are two of them: anandamide (named from the Sanskrit word for bliss) and 2-arachidonoyl glycerol.
The building blocks of the endocannabinoids are stored within the postsynaptic neurons. When an NT activates the postsynaptic neuron, it starts a process that synthesizes endocannabinoids and spits them out into the synaptic space. These endocannabinoids then travel backwards, or upstream, to the presynaptic neuron, where specialized cannabinoid receptors are located. (There are two cannabinoid receptors, called CB1 and CB2. The CB1 receptors live mainly in the brain, while the CB2 receptors are in the immune system.) Once the endocannabinoids bind to the cannabinoid receptors, they act to inhibit the neuron from firing. The process is known as “retrograde transmission” and causes “presynaptic inhibition”—ie, reduced NT release.
In other words, a primary function of the ECS is to buffer the brain’s NT activity. This buffering process affects both excitatory (mainly glutamatergic) and inhibitory (mainly GABAergic) circuits. Putting the brakes on a glutamate neuron slows things down. But inhibiting a GABA neuron means reducing inhibition, so it speeds things up. Some researchers think that this dual effect helps to explain the various paradoxical psychoactive effects of cannabis: For example, the drug causes drowsiness on the one hand but enhances sensory experience on the other; it decreases anxiety at low doses but worsens it at higher doses.
This brings us right into the next topic—how does THC affect the ECS?
THC’s effect on the ECS
When someone uses marijuana, THC insinuates itself throughout the user’s ECS, latching onto cannabinoid receptors all over the brain and crowding out endocannabinoids. What does this mean for perception, emotion, and behavior? That depends on which parts of the brain we’re talking about.
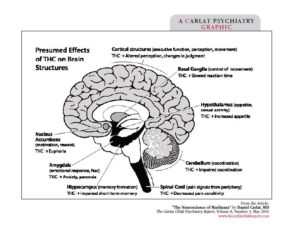
Graphic: Presumed Effects of THC on Brain Structures
(Click Here To View Full Size PDF.)
This figure shows brain structures that are loaded with cannabinoid receptors and therefore especially vulnerable to the effects of THC. The psychoactive effects of THC match up pretty neatly with specific brain structures. For example, pot’s impairment of short-term memory is likely due to THC slowing down neurotransmission in the hippocampus, where we normally create memories. Its usefulness for chronic pain may be an effect of influencing transmission in the spinal cord.
An interesting side note (one that should make all stoners happy) is that there are no cannabinoid receptors in the brain stem, which is responsible for respiration. This means high doses of pot do not cause respiratory depression and death—unlike opioid overdoses.
The bottom line for your patients
How can you use your knowledge of the ECS in your interactions with teenage pot smokers? Tell patients that we now know a lot about how pot works in specific areas of the brain. They will be fascinated that the brain makes its own cannabinoids to keep itself functioning smoothly. However, non-endogenous cannabinoids, such as THC, throw this system off kilter. If this happens occasionally, little if any harm is done. However, constant use—or perhaps use at critical periods of brain development, such as early adolescence—is apt to spark long-term effects such as poorer motivation and difficulty learning and remembering information.
Will sharing this simplified version of marijuana neuroscience have an impact on your patients? You won’t know unless you try. (For more information, see Journal of Psychoactive Drugs January–March 2016;48(1).)


Recommended


