
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
Disruptive Mood Dysregulation Disorder: A Primer
Nine-year-old Johnny has had chronic grouchiness and severe temper outbursts since early childhood. At age 4, Johnny was asked to leave preschool because of his behavior and was diagnosed with ADHD. Stimulant treatment diminished the ADHD symptoms a lot and the irritability a bit. Johnny continued to have both chronic grouchiness and outbursts when frustrated; these occurred daily at home and weekly at school. Most outbursts were verbal, but some were physical. Most recently, he has been diagnosed with disruptive mood dysregulation disorder (DMDD), a new diagnosis unveiled in 2013 in DSM-5. His therapist and his child psychiatrist have tried a number of treatments. Parent training therapy seemed to help at first, but the behaviors returned. Both SSRIs and atypical antipsychotic treatment have been somewhat effective, but the antipsychotic caused significant sedation and weight gain.
Chronic irritability: An evolving perspective
In the 1990s and early 2000s, many clinicians might have diagnosed Johnny with bipolar disorder (BD). This might have happened even though the diagnosis would not have been justifiable using DSM-IV criteria, since Johnny had never had a manic episode. At the time, many child psychiatrists thought that pediatric BD presented with chronic irritability and symptoms of ADHD, rather than with the distinct manic episodes that characterize adult BD. Research subsequently showed that chronic irritability is not how BD presents in children (Leibenluft E, Am J Psychiatry 2011;168(2):129–142). As it turns out, chronically irritable children are not at increased risk to develop manic episodes as they age; instead, they are at increased risk for anxiety and unipolar depression later in life. Moreover, unlike children with BD, chronically irritable children do not tend to have unusually strong family histories of BD. Rather, there are both genetic and familial links between chronic irritability and unipolar depression.
This research created a quandary. Clearly, there are many children who are chronically irritable and who tend to develop depression and not mania. They suffer just as much as children with BD, but under DSM-IV, there wasn’t a distinct diagnosis for very severe, chronic irritability—a disturbance in mood—as the major problem. In an attempt to remedy this issue, the authors of DSM-5 included disruptive mood dysregulation disorder (DMDD) as a new diagnosis (Towbin K et al, J Am Acad Child Adolesc Psychiatry 2013;52:466–481).
Assessment and diagnosis
Irritability is among the most common reasons children are referred for psychiatric evaluation and care. In community studies, prevalence rates of severe irritability in children range from 2% to 5%. It is likely that you have and will see children with DMDD, possibly without recognizing them, so it is important to know how to make this diagnosis.
Johnny’s case illustrates the two core criteria for DMDD: temper outbursts and a generally irritable mood. The temper outbursts have to occur, on average, at least three times a week. Although temper outbursts are a common feature of many psychiatric illnesses, not many children have three outbursts a week on a regular basis. Some clinicians think that the outbursts in DMDD must have a physical component, but this is not true. In fact, the most common features of temper outbursts seen in youth with DMDD include yelling, screaming, or verbally threatening someone, without any physical components. For the DMDD diagnosis, your patient’s temper outbursts can be verbal (as most of Johnny’s were) and/or physical. Seriously consider the DMDD diagnosis if your patient is verbally argumentative, snappy, and apt to engage in name calling more frequently, intensely, and persistently than typical for someone that age.
Of course, most DMDD youth have occasional physical outbursts, even if their more typical outbursts are verbal. Physical temper outbursts can include slamming a door, throwing something down, kicking furniture, physically threatening someone (eg, clenching fists, raising an arm to hit), or destroying property (eg, kicking a hole in a wall, breaking belongings). The most severe (and rarest) temper outbursts cause harm towards another person. These behaviors include intentionally throwing an object directly at someone or physically pushing, shoving, slapping, or kicking someone.
The second core criterion for DMDD is pervasive irritable mood. To assess this, we ask parents whether they (and others) generally see the child as grouchy and grumpy. Caregivers of youth with DMDD often say they feel like they have to “walk on eggshells” for fear of upsetting their generally angry child. Throughout the day, the child is cranky and crabby, and the people in the child’s life see the child that way. When you assess a child for major depressive disorder, you have to determine whether the child is sad “most days most of the time.” For DMDD, it’s a very similar assessment; but, rather than focusing on sadness, you have to decide whether the child is cranky and crabby most of the time.
It’s important to note that parents often avoid certain activities (like going out to a restaurant or inviting another family to visit) and avoid asking the child to do things that they ask of the child’s siblings, such as homework or chores. If the parent accommodates the child by making very few requests in order to avoid an outburst and keep the child’s irritability under control, this should be noted. For example, some children will exhibit two outbursts per week, below the frequency criterion for DMDD, but parents will avoid making normal demands on the child and will refrain from enforcing a request in order to avoid or terminate an outburst. In these instances, the child meets the diagnostic criterion for DMDD. This is analogous to what you would do when you are assessing avoidance in a child with a possible anxiety disorder and there is substantial parental accommodation. Even if a child does not overtly express avoidance, you would still diagnose a child with anxiety disorder if the parents make accommodations that remove any opportunity for the child to either confront or avoid a feared object. The situation with DMDD is the same.
In DMDD, irritable mood has to be present for at least a year, but usually the mood has been present for much longer than that. Again, like temper outbursts, many children with psychiatric problems present with irritability. However, only a subset of these children will have persistent irritability that is present most days for a year, as is required for DMDD.
Importantly, the temper outbursts and pervasive, persistent crankiness of children with DMDD inhibit their ability to get along at home, at school, and with their friends. Indeed, the DSM-5 criteria for DMDD require that the child’s irritability be severely impairing in at least one of these three settings, and at least mildly impairing in a second setting. If parents or teachers make accommodations in an attempt to diminish the child’s irritability, this would be evidence of impairment.
Treatment
We usually look to large randomized controlled trials (RCTs) to decide on best treatments. Unfortunately, no such trials exist for the treatment of DMDD. As a result, you cannot make strong recommendations to patients and families regarding any particular treatment. Instead, your recommendations can be guided only by indirect evidence on safety and efficacy. This evidence derives from RCTs on disorders related to DMDD and from small, open trials in DMDD. To treat your patient with DMDD, it is important for you to know the relevant data on psychotherapy, medications, and experimental treatments.
Psychotherapy
When selecting a treatment, you might consider psychotherapy first. This is because evidence on efficacy for problems similar to DMDD, like aggression, is as strong, or stronger, than the evidence for any other treatment, and because psychotherapy is relatively noninvasive. Moreover, open trials of psychotherapy for DMDD itself show promise.
Parent training involves reinforcing pro-social behavior and using time-outs to extinguish emotional outbursts (Patterson GR. Families: Applications of Social Learning to Family Life. Champaign, IL: Research Press; 1975). These techniques work for various conduct problems, and early evidence suggests that they may also decrease the temper outbursts of DMDD.
Components of cognitive behavioral therapy (CBT) may also be helpful, based on research in pediatric mood, anxiety, and behavior disorders (Waxmonsky JG et al, J Am Acad Child Adolesc Psychiatry 2016;55(3):196–207). These techniques teach children how to regulate their emotions and how to focus their attention away from negative experiences.
Medication
Like psychotherapies, various medications have been shown to reduce temper outbursts or irritability in children being treated for disorders other than DMDD. In the absence of data from RCTs directly targeting DMDD, however, we can only use indirect evidence to guide treatment choice.
Psychostimulants
In line with Johnny’s experience, data suggests that psychostimulants reduce features of DMDD in children with ADHD, despite earlier concerns based on anecdotal evidence to the contrary (Fernandez de la Cruz L et al, J Am Acad Child Adolesc Psychiatry 2015;54(1):62–70). If you do decide to try medications for your DMDD patient, stimulants’ long record of safety and rapid clinical effects on core ADHD symptoms make them a reasonable first choice.
Selective serotonin reuptake inhibitors (SSRIs)
SSRIs have been shown in large RCTs to reduce many features of pediatric anxiety and depressive disorders. Since anxiety and depression are often linked with irritability, it makes intuitive sense that SSRIs would be helpful for the irritability component of DMDD. Data in adults suggests that SSRIs reduce the irritability associated with depressive disorders, but conclusive data in children is more limited—more research is ongoing at the NIMH.
You might have concerns about SSRIs causing mania in patients with DMDD. Data from open trials of SSRIs for DMDD suggests that the risk of medication-induced mania is quite low, but there’s not enough data to estimate the risk level. We also know that SSRIs can cause activation or suicidal ideation in children, probably including those with DMDD, although there is a paucity of research.
Antipsychotics
Antipsychotics are usually less well tolerated than SSRIs, since they cause adverse metabolic and neurological effects, especially when used for long periods of time. This is consistent with Johnny’s experience, described earlier. On the other hand, we have more data showing the effectiveness of antipsychotics on irritability in other conditions such as autism spectrum disorders and disruptive behavior disorders. As with SSRIs, you should consider antipsychotics reasonable second-line medication choices in the treatment of DMDD.
Interestingly, one small RCT found that lithium did no better than placebo in treating children with DMDD, which is consistent with longitudinal data suggesting that DMDD is not a pediatric manifestation of bipolar disorder.
Experimental treatments
Researchers at the NIMH are now testing whether computer-based training can decrease irritability in youth with DMDD. This technique trains children to not interpret ambiguous facial expressions as angry (Stoddard J et al, J Child Adolesc Psychopharmacology 2016;26(1):49–57). This is based on research throughout the 1990s linking “hostile attribution bias” to aggression in children (Crick NR and Dodge KA, Child Development 1996;67(3):993–1002). This NIMH research includes brain imaging, which might help to identify the brain circuits involved in irritability and guide the development of this and other new treatments.
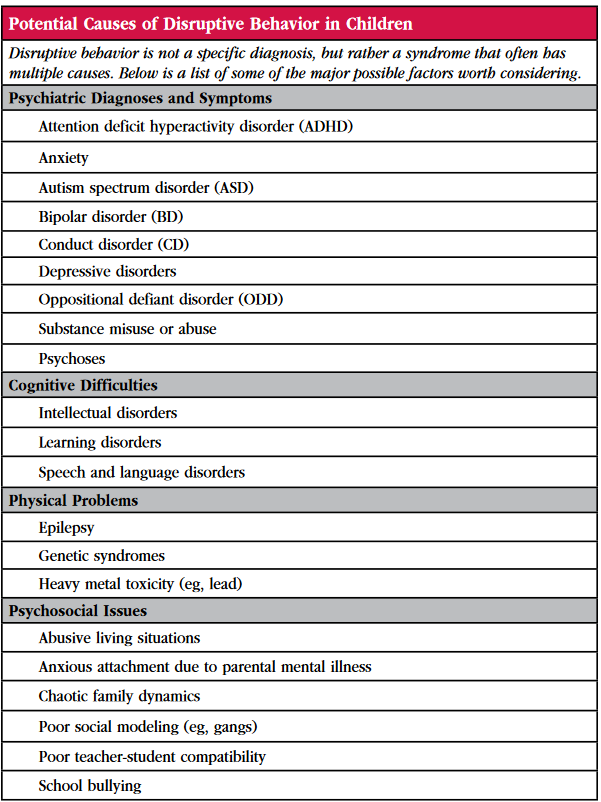
Table: Potential Causes of Disruptive Behavior in Children
NIMH Clinical Trials on DMDD
Dr. Leibenluft and her colleagues are conducting several research projects at the Emotion and Development Branch at NIMH that might be of interest to your patients. For further information, contact: irritablekids@mail.nih.gov or 301-496-8381. Potential subjects would be screened for DMDD criteria and might be eligible to enroll in one of several studies underway: 1. Efficacy of CBT and parent training to treat youth with DMDD; 2. SSRI effects on DMDD; and 3. Other novel treatment interventions for DMDD.


Recommended


