
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
The New(er) Drugs for Alcoholism
Reviewing the new medications for alcoholism brings us into a pharmacologic netherworld. Nothing is very clear, and when you think you've finally come to a conclusion, a new study comes along to cast a fresh fog over everything.
We'll start with naltrexone (brand name ReVia), currently the only medication other than Antabuse (disulfiram) to be FDA-approved for alcoholism. Naltrexone blocks opiate receptors, and presumably helps prevent relapse by depriving the drinker of a secondary opiate-induced "buzz" that would normally lead to a craving for more. It's a longer-acting version of Narcan, which is used to quickly revive drug users from a heroininduced stupor in the ER.
The first big naltrexone paper came out with much fanfare in 1992 (Arch Gen Psychiatry 1992;49:876- 880), and showed that after 12 weeks of treatment, only 23% of hard core VA alcoholics relapsed vs. 54% of those receiving placebo. A second positive study led to FDA approval, but since then, results have been mixed. Some of these contrary results were explained away because they came out of Europe, where patients enter clinical trials after a period of abstinence and tend not to be addicted to other substances as well. Thus, they may be less "severe" than the American subjects and thus less responsive to the effects of naltrexone.
Unfortunately, a large negative U.S. trial was published 3 years ago from a VA system, looking at 600 patients, who were randomly assigned to one of three arms: 12 months of naltrexone (50 mg daily); three months of naltrexone followed by nine months of placebo; or 12 months of placebo (N Engl J Med 2001;345:1734-1739). The results? No difference at all among the three groups, in rate of relapse or percentage of drinking days.
So is naltrexone a fancy placebo after all? Many researchers are still standing by their med, but the recent data do not impress.
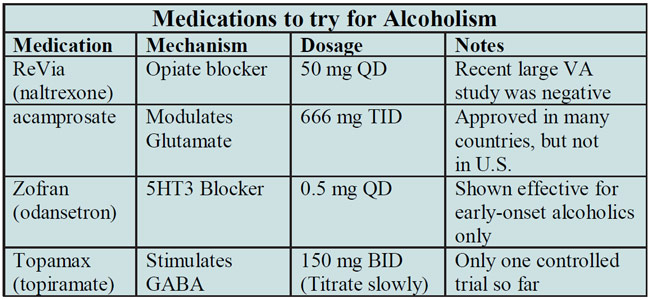
Table: Medications to try for Alcoholism
Acamprosate. Europe has been much kinder to acamprosate than it has to naltrexone. Fourteen of sixteen controlled trials have shown it to be effective for reducing drinking (Med J Aust 2002;177:103-107), and it is an approved medication for alcoholism throughout Europe and Latin America.
Back here in the US of A, the FDA’s Psychopharmacological Drugs Advisory Board voted by an 8 to 2 margin that acamprosate is indeed effective at promoting sobriety, but nonetheless the FDA issued a “nonapprovable letter” to Forest pharmaceuticals in July 2002. Apparently, an unpublished U.S. trial comparing acamprosate to placebo was unimpressive, and the FDA wants to see more data. Experts in the field are fairly certain that it will gain approval eventually.
How does acamprosate work? By calming down the glutamate system, which becomes overly excitable as a result of chronic alcohol abuse. Too much glutamate activity seems to be one of the things driving alcoholics toward that next drink.
Acamprosate is extremely well-tolerated, with much milder GI side effects than naltrexone, and no liver toxicity. One weird thing about it is that it comes in 333 mg tablets, and the recommended daily dose is a bizarre "1998 mg" per day. To make matters worse, it's supposed to be dosed as 2 tablets TID. As compared to this byzantine dosing schedule, naltrexone's a breeze at 50 mg a day, period.
It may be that combining acamprosate with naltrexone is the way to go. A recent Archives of General Psychiatry article showed a relapse rate of only 25% on the combination therapy 12 weeks after detox, as compared to 50-60% relapse rates on naltrexone or acamprosate alone (Arch Gen Psych 2003;60:92-99).
Zofran (odansetron). Zofran is the fabulously expensive anti-emetic used for treating nausea induced by chemotherapy in cancer patients. Over the years, it has wended its way into alcoholism research, largely because it blocks 5HT 3 receptors, and any medication that touches serotonin is fair game for any indication in psychiatry. It so happens that most of the serotonin data in alcoholics implies a serotonin deficiency, which would not logically endorse a serotonin-blocking drug like Zofran, but such technicalities can be massaged away by using terms in research papers such as "serotonin modulation" and the like.
A single controlled trial of Zofran in alcoholics has been published (JAMA 2000;284:963-971) and showed that it modestly reduced drinking relative to placebo, but only in the early-onset group. "Earlyonset" alcoholics, also known in the field as "Type II" or "Type B" alcoholics, have onset before age 25, have a strong family history of alcoholism, and have antisocial personality traits. The optimal dose was less than 0.5 mg QD, which can only be achieved by prescribing the oral solution (4 mg/5 ml). It's worth a try when nothing else works.
Topamax. Yes, Topamax (topiramate), the drug that everybody wishes would work for everything (because it causes weight loss as a side effect--see TCR 1:9) has been tested in alcoholism and seems to beat placebo (Lancet 2003;361:1677). 150 alcoholic men and women were randomised to either Topamax or placebo; all patients also received weekly 20 minute brief therapy sessions with study nurses who were blind to the treatment. In the Topamax group, the dose was titrated up very gradually to 150 mg BID. On the average, Topamax patients had significantly fewer drinks and more days of abstinence than the placebo group at the 12 week endpoint.
TCR VERDICT:
Meds for Alcoholism: We’re far from Panacea
General PsychiatryWe'll start with naltrexone (brand name ReVia), currently the only medication other than Antabuse (disulfiram) to be FDA-approved for alcoholism. Naltrexone blocks opiate receptors, and presumably helps prevent relapse by depriving the drinker of a secondary opiate-induced "buzz" that would normally lead to a craving for more. It's a longer-acting version of Narcan, which is used to quickly revive drug users from a heroininduced stupor in the ER.
Naltrexone has disappointed; Acamprosate is seeking FDA approval
The first big naltrexone paper came out with much fanfare in 1992 (Arch Gen Psychiatry 1992;49:876- 880), and showed that after 12 weeks of treatment, only 23% of hard core VA alcoholics relapsed vs. 54% of those receiving placebo. A second positive study led to FDA approval, but since then, results have been mixed. Some of these contrary results were explained away because they came out of Europe, where patients enter clinical trials after a period of abstinence and tend not to be addicted to other substances as well. Thus, they may be less "severe" than the American subjects and thus less responsive to the effects of naltrexone.
Unfortunately, a large negative U.S. trial was published 3 years ago from a VA system, looking at 600 patients, who were randomly assigned to one of three arms: 12 months of naltrexone (50 mg daily); three months of naltrexone followed by nine months of placebo; or 12 months of placebo (N Engl J Med 2001;345:1734-1739). The results? No difference at all among the three groups, in rate of relapse or percentage of drinking days.
So is naltrexone a fancy placebo after all? Many researchers are still standing by their med, but the recent data do not impress.
Table: Medications to try for Alcoholism
Acamprosate. Europe has been much kinder to acamprosate than it has to naltrexone. Fourteen of sixteen controlled trials have shown it to be effective for reducing drinking (Med J Aust 2002;177:103-107), and it is an approved medication for alcoholism throughout Europe and Latin America.
Back here in the US of A, the FDA’s Psychopharmacological Drugs Advisory Board voted by an 8 to 2 margin that acamprosate is indeed effective at promoting sobriety, but nonetheless the FDA issued a “nonapprovable letter” to Forest pharmaceuticals in July 2002. Apparently, an unpublished U.S. trial comparing acamprosate to placebo was unimpressive, and the FDA wants to see more data. Experts in the field are fairly certain that it will gain approval eventually.
How does acamprosate work? By calming down the glutamate system, which becomes overly excitable as a result of chronic alcohol abuse. Too much glutamate activity seems to be one of the things driving alcoholics toward that next drink.
Acamprosate is extremely well-tolerated, with much milder GI side effects than naltrexone, and no liver toxicity. One weird thing about it is that it comes in 333 mg tablets, and the recommended daily dose is a bizarre "1998 mg" per day. To make matters worse, it's supposed to be dosed as 2 tablets TID. As compared to this byzantine dosing schedule, naltrexone's a breeze at 50 mg a day, period.
It may be that combining acamprosate with naltrexone is the way to go. A recent Archives of General Psychiatry article showed a relapse rate of only 25% on the combination therapy 12 weeks after detox, as compared to 50-60% relapse rates on naltrexone or acamprosate alone (Arch Gen Psych 2003;60:92-99).
Zofran (odansetron). Zofran is the fabulously expensive anti-emetic used for treating nausea induced by chemotherapy in cancer patients. Over the years, it has wended its way into alcoholism research, largely because it blocks 5HT 3 receptors, and any medication that touches serotonin is fair game for any indication in psychiatry. It so happens that most of the serotonin data in alcoholics implies a serotonin deficiency, which would not logically endorse a serotonin-blocking drug like Zofran, but such technicalities can be massaged away by using terms in research papers such as "serotonin modulation" and the like.
A single controlled trial of Zofran in alcoholics has been published (JAMA 2000;284:963-971) and showed that it modestly reduced drinking relative to placebo, but only in the early-onset group. "Earlyonset" alcoholics, also known in the field as "Type II" or "Type B" alcoholics, have onset before age 25, have a strong family history of alcoholism, and have antisocial personality traits. The optimal dose was less than 0.5 mg QD, which can only be achieved by prescribing the oral solution (4 mg/5 ml). It's worth a try when nothing else works.
Topamax. Yes, Topamax (topiramate), the drug that everybody wishes would work for everything (because it causes weight loss as a side effect--see TCR 1:9) has been tested in alcoholism and seems to beat placebo (Lancet 2003;361:1677). 150 alcoholic men and women were randomised to either Topamax or placebo; all patients also received weekly 20 minute brief therapy sessions with study nurses who were blind to the treatment. In the Topamax group, the dose was titrated up very gradually to 150 mg BID. On the average, Topamax patients had significantly fewer drinks and more days of abstinence than the placebo group at the 12 week endpoint.
TCR VERDICT:
Meds for Alcoholism: We’re far from Panacea



Recommended


