
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
Treating Alcohol Use Disorder
 Albert J. Arias, MD, MS
Albert J. Arias, MD, MSAssociate Professor, Psychiatry Virginia Commonwealth University School of Medicine. Associate Division Chair, Addiction Psychiatry and Addiction Medicine. Dr. Arias has disclosed that he has no relevant financial or other interests in any commercial companies pertaining to this educational activity.
CATR: Can you tell us about the role of medications for alcohol use disorder (AUD)?
Dr. Arias: Medications are a very important part of AUD treatment. They can and should be used as a first-line treatment in any reasonable medical setting—primary care or psychiatry, or a specialty addiction setting. Unfortunately, very few patients ever receive them. The reasons for that are complicated, but some of it has to do with doctors not being comfortable with prescribing these meds, even though they are not difficult to use.
CATR: So, we shouldn’t reserve medications for people who have failed psychotherapy or AA.
Dr. Arias: Exactly. Medications are a first-line treatment for AUD, and they can also be used as a monotherapy, although there is certainly nothing wrong with adding evidence-based psychotherapy or mutual help. Whether or not people really do better with both is still a question, but I think from a practical perspective we should approach these problems from a patient-centered angle and see what people are willing to do.
CATR: Could you tell us about the specific medications?
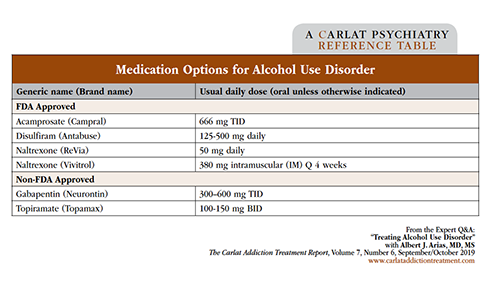
Dr. Arias: We have five main agents. Three are FDA approved: naltrexone (oral and extended release), acamprosate, and disulfiram. And then we also have topiramate and gabapentin. All these meds have a reasonable evidence base, though some stronger than others. Disulfiram probably has the weakest evidence for efficacy, but it has been shown to be effective under certain conditions. (See table below covering medication options for alcohol dependence.)
CATR: Any advice on how to choose between these medications?
Dr. Arias: You want to start with a biopsychosocial assessment and then address the patient’s goals. I find that a lot of people are concerned about side effects, so starting with acamprosate or gabapentin or naltrexone is a good way to go. The thing to consider is that naltrexone may work best on reducing measures of heavy drinking (ie, delaying the time to relapse to heavy drinking, and reducing the amount of heavy drinking, the proportion of patients returning to heavy drinking, the percent days heavy drinking, and drinking quantity), whereas acamprosate primarily targets abstinence measures (ie, abstinence rate, percent days abstinent, and time to first drink). It’s good for the clinician to know what to expect in terms of each medication’s effects on drinking, and to discuss that with the patient to make sure the patient knows what to expect and to see if the effects match the patient’s goals. Another thing to consider is adherence: Naltrexone is usually given once a day, or in a monthly injection, whereas acamprosate needs to be taken 3 times a day. I also tell patients about topiramate; however, I’m up front with them about the possible paresthesia and cognitive side effects, and the long titration, and usually they will agree that it is probably worth trying one of the other meds first.
CATR: What about disulfiram? Do you reserve it for a certain subset of patients?
Dr. Arias: I usually won’t use disulfiram in patients who have significant heart or liver disease, because of the risk of the disulfiram reaction and the strain that it can put on the body, in addition to potential hepatotoxicity. I will also tell patients, “The evidence is not generally good for this medication, because people tend to not take it or stop taking it.” However, this is where the biopsychosocial evaluation can come in handy, because some of the evidence for the effectiveness of disulfiram is in settings where a patient has somebody (usually a family member) to help with medication adherence, or in situations where it can be essentially mandated—for example, as a required part of a patient’s methadone treatment if the patient has opioid and alcohol use disorders.
CATR: Clinicians sometimes have doubts about acamprosate. Does it actually work?
Dr. Arias: There’s a good meta-analysis, and though it’s not clear that acamprosate reduces heavy drinking, it does delay relapse and increases abstinence rates and other abstinence measures (Maisel NC et al, Addiction 2013;108(2):275–293). It’s a good medication for people who want to try to be mostly abstinent. The authors of the meta-analysis looked at patients’ stated goals whenever possible, and those goals weren’t a significant moderator of either naltrexone or acamprosate. But despite that, I think it’s reasonable to reserve acamprosate for patients who want to be abstinent. I have tried it with some patients who don’t have abstinence as a goal, and I don’t think it works effectively in those patients. But I have seen it work in people who are trying to mostly not drink. And even if they slip, they can get back on track more easily. But in general, the actual effect size is small, which is also true of naltrexone and disulfiram.
CATR: Topiramate, from what I understand, may be the most effective of these five medications. Is that correct?
Dr. Arias: Yes, there have been good trials showing that it works well. The effect holds up in meta-analysis, and it seems to have a moderate effect size for increasing abstinence measures and reducing heavy drinking (Blodgett JC et al, Alcohol Clin Exp Res 2014;38(6):1481–1488). There are several other potential advantages to topiramate, but there also are some drawbacks. One of the main advantages is that it has been shown to work in people who are regularly drinking heavily without any specified period of abstinence prior to treatment. The other medications may work in those people also; however, we know that for naltrexone and acamprosate, the effect size is much smaller if patients are unable to get at least several days to a week of sobriety. Topiramate seems to work for a wide spectrum of patients, and in my experience, it may help in patients who have impulsivity or anxiety. I certainly have seen it work in people who don’t respond to other medications.
CATR: Is there any benefit in combining any of these medications?
Dr. Arias: The best evidence is for combining naltrexone and gabapentin. There’s a good trial done at MUSC in which gabapentin added to naltrexone was better than either drug alone (Anton RF et al, Am J Psychiatry 2011;168(7):709–717). We don’t want to rely too much on one trial even if it was well done, but in my experience that’s how I use gabapentin—I may start it in the detox window for subjective symptoms of withdrawal, then add naltrexone, then keep the patient on the combination. In my experience, that’s where it will be more effective in reducing the risk of return to harmful drinking: in combination rather than just as monotherapy. There have been other studies suggesting benefits of combining other medications, although the results are mixed, and a large study of naltrexone combined with acamprosate showed no advantage of combining the two (Anton RF et al, JAMA 2006;295(17):2003–2017).
CATR: How long should we keep patients on medications for AUD?
Dr. Arias: The evidence suggests that there are people who may benefit from continued medication treatment at a year or more. And at the same time, there are some studies that show, for example, with topiramate that people may have sustained benefits after just being treated for 12 weeks (Kranzler HR et al, Alcohol Clin Exp Res 2014;38(12):3017–3023). My approach is that there isn’t a preordained optimal time for any one patient, and I suggest that people consider doing the treatment for about 6 months. Then, if they feel so inclined, we can consider stopping the medication at that point, or they could stay on it for a year or up to 2 years, at which point we should consider on a case-by-case basis whether it makes sense to continue or not.
CATR: What if there is no reduction in drinking? When do you feel that it’s time to stop the medication and switch to another one?
Dr. Arias: Six weeks on the medication is probably adequate, and with topiramate I would start counting after patients have reached a good target dose of 200–300 mg a day. Usually I will go up to 300 mg if they can tolerate it, and if in 4–6 weeks they haven’t improved, then it’s probably not going to work.
CATR: We sometimes hear about the use of these meds for people who have not yet developed a full AUD.
Dr. Arias: Right. There’s evidence that you can consider medications for people who drink too much but haven’t yet developed a full-blown AUD. And naltrexone can also be used in a targeted “as needed” way to prevent binge drinking when a patient is going to a certain event, such as a wedding, and is concerned about having a binge. The patient would take the naltrexone a couple of hours ahead of the event.
CATR: Let’s switch gears a bit and talk about the role of psychotherapy. The depression analogy comes up: We know that cognitive behavioral therapy (CBT) works, as do meds, but the combination may be better than either one alone. Is that true for AUD?
Dr. Arias: It’s not clear that it’s true for AUD. The literature supports the use of medications as well as certain psychotherapies as efficacious treatments; however, it’s not clear that adding psychotherapy to medications improves outcomes above medication by itself. Clinically, it pays to have a patient-centered approach and think about what’s going on with your patient’s specific case. There may be some advantages to therapy that the patient isn’t necessarily going to get with the medication, and vice versa.
CATR: In terms of outcomes, we used to think of abstinence. How should we think of outcomes nowadays?
Dr. Arias: For a long time this has been controversial, but recently there has been work that clearly frames reduction in drinking as a desired and sufficient outcome. There are some patients, usually because of the severity of their AUD or their comorbidities, who have very little control once they resume drinking. So, for some people there is reason to get them to try to be totally abstinent. But for most people, insisting on abstinence is probably just going to drive them out of treatment and break the therapeutic alliance.
CATR: So, reducing drinking is a reasonable outcome for most patients.
Dr. Arias: Exactly. There is a recent analysis looking at the World Health Organization’s drinking risk categories, and it shows that reducing a person’s risk category by at least 1 or preferably 2 levels is associated with much better overall outcomes (Witkiewitz K et al, Alcohol Clin Exp Res 2017;41(1):179–186). That may mean some people are still drinking a couple of times a week, maybe even drinking heavily on some days. But if they’ve substantially reduced their drinking, their health will be much improved. And that is concordant with a previous analysis using traditional abstinence and no heavy drinking outcomes, where it was shown that, while no heavy drinking is the best, there’s not a huge difference between heavy drinking occasionally and no heavy drinking.
CATR: We still have this idea that the first step is doing a detox. But we now know that most people go back to drinking. Is it worth recommending detox if we are rethinking outcomes in terms of reduction in drinking?
Dr. Arias: I don’t think we should give up detoxing entirely, but I think there may be people where insisting on detox first isn’t necessary. And since we now have at least one medication like topiramate that probably works well even if people are regularly drinking heavily and have mild withdrawal, we may be able to skip detox in some of those people. What I find is that clinically, there’s a certain point where people who drink heavily have induced a state that they really can’t safely go a day without drinking. So, I think we should shift toward assessing the severity of withdrawal and stratifying risk and the need for medically supervised detox. There are now some valid instruments that may help with the task, such as the Prediction of Alcohol Withdrawal Severity Scale (PAWSS) (Maldonado JR et al, Alcohol and Alcoholism 2015;50(5):509–518).
CATR: Thank you for your time, Dr. Arias.
Addiction TreatmentDr. Arias: Medications are a very important part of AUD treatment. They can and should be used as a first-line treatment in any reasonable medical setting—primary care or psychiatry, or a specialty addiction setting. Unfortunately, very few patients ever receive them. The reasons for that are complicated, but some of it has to do with doctors not being comfortable with prescribing these meds, even though they are not difficult to use.
CATR: So, we shouldn’t reserve medications for people who have failed psychotherapy or AA.
Dr. Arias: Exactly. Medications are a first-line treatment for AUD, and they can also be used as a monotherapy, although there is certainly nothing wrong with adding evidence-based psychotherapy or mutual help. Whether or not people really do better with both is still a question, but I think from a practical perspective we should approach these problems from a patient-centered angle and see what people are willing to do.
CATR: Could you tell us about the specific medications?
Dr. Arias: We have five main agents. Three are FDA approved: naltrexone (oral and extended release), acamprosate, and disulfiram. And then we also have topiramate and gabapentin. All these meds have a reasonable evidence base, though some stronger than others. Disulfiram probably has the weakest evidence for efficacy, but it has been shown to be effective under certain conditions. (See table below covering medication options for alcohol dependence.)
Click to view full-size PDF.
CATR: Any advice on how to choose between these medications?
Dr. Arias: You want to start with a biopsychosocial assessment and then address the patient’s goals. I find that a lot of people are concerned about side effects, so starting with acamprosate or gabapentin or naltrexone is a good way to go. The thing to consider is that naltrexone may work best on reducing measures of heavy drinking (ie, delaying the time to relapse to heavy drinking, and reducing the amount of heavy drinking, the proportion of patients returning to heavy drinking, the percent days heavy drinking, and drinking quantity), whereas acamprosate primarily targets abstinence measures (ie, abstinence rate, percent days abstinent, and time to first drink). It’s good for the clinician to know what to expect in terms of each medication’s effects on drinking, and to discuss that with the patient to make sure the patient knows what to expect and to see if the effects match the patient’s goals. Another thing to consider is adherence: Naltrexone is usually given once a day, or in a monthly injection, whereas acamprosate needs to be taken 3 times a day. I also tell patients about topiramate; however, I’m up front with them about the possible paresthesia and cognitive side effects, and the long titration, and usually they will agree that it is probably worth trying one of the other meds first.
CATR: What about disulfiram? Do you reserve it for a certain subset of patients?
Dr. Arias: I usually won’t use disulfiram in patients who have significant heart or liver disease, because of the risk of the disulfiram reaction and the strain that it can put on the body, in addition to potential hepatotoxicity. I will also tell patients, “The evidence is not generally good for this medication, because people tend to not take it or stop taking it.” However, this is where the biopsychosocial evaluation can come in handy, because some of the evidence for the effectiveness of disulfiram is in settings where a patient has somebody (usually a family member) to help with medication adherence, or in situations where it can be essentially mandated—for example, as a required part of a patient’s methadone treatment if the patient has opioid and alcohol use disorders.
CATR: Clinicians sometimes have doubts about acamprosate. Does it actually work?
Dr. Arias: There’s a good meta-analysis, and though it’s not clear that acamprosate reduces heavy drinking, it does delay relapse and increases abstinence rates and other abstinence measures (Maisel NC et al, Addiction 2013;108(2):275–293). It’s a good medication for people who want to try to be mostly abstinent. The authors of the meta-analysis looked at patients’ stated goals whenever possible, and those goals weren’t a significant moderator of either naltrexone or acamprosate. But despite that, I think it’s reasonable to reserve acamprosate for patients who want to be abstinent. I have tried it with some patients who don’t have abstinence as a goal, and I don’t think it works effectively in those patients. But I have seen it work in people who are trying to mostly not drink. And even if they slip, they can get back on track more easily. But in general, the actual effect size is small, which is also true of naltrexone and disulfiram.
CATR: Topiramate, from what I understand, may be the most effective of these five medications. Is that correct?
Dr. Arias: Yes, there have been good trials showing that it works well. The effect holds up in meta-analysis, and it seems to have a moderate effect size for increasing abstinence measures and reducing heavy drinking (Blodgett JC et al, Alcohol Clin Exp Res 2014;38(6):1481–1488). There are several other potential advantages to topiramate, but there also are some drawbacks. One of the main advantages is that it has been shown to work in people who are regularly drinking heavily without any specified period of abstinence prior to treatment. The other medications may work in those people also; however, we know that for naltrexone and acamprosate, the effect size is much smaller if patients are unable to get at least several days to a week of sobriety. Topiramate seems to work for a wide spectrum of patients, and in my experience, it may help in patients who have impulsivity or anxiety. I certainly have seen it work in people who don’t respond to other medications.
CATR: Is there any benefit in combining any of these medications?
Dr. Arias: The best evidence is for combining naltrexone and gabapentin. There’s a good trial done at MUSC in which gabapentin added to naltrexone was better than either drug alone (Anton RF et al, Am J Psychiatry 2011;168(7):709–717). We don’t want to rely too much on one trial even if it was well done, but in my experience that’s how I use gabapentin—I may start it in the detox window for subjective symptoms of withdrawal, then add naltrexone, then keep the patient on the combination. In my experience, that’s where it will be more effective in reducing the risk of return to harmful drinking: in combination rather than just as monotherapy. There have been other studies suggesting benefits of combining other medications, although the results are mixed, and a large study of naltrexone combined with acamprosate showed no advantage of combining the two (Anton RF et al, JAMA 2006;295(17):2003–2017).
CATR: How long should we keep patients on medications for AUD?
Dr. Arias: The evidence suggests that there are people who may benefit from continued medication treatment at a year or more. And at the same time, there are some studies that show, for example, with topiramate that people may have sustained benefits after just being treated for 12 weeks (Kranzler HR et al, Alcohol Clin Exp Res 2014;38(12):3017–3023). My approach is that there isn’t a preordained optimal time for any one patient, and I suggest that people consider doing the treatment for about 6 months. Then, if they feel so inclined, we can consider stopping the medication at that point, or they could stay on it for a year or up to 2 years, at which point we should consider on a case-by-case basis whether it makes sense to continue or not.
CATR: What if there is no reduction in drinking? When do you feel that it’s time to stop the medication and switch to another one?
Dr. Arias: Six weeks on the medication is probably adequate, and with topiramate I would start counting after patients have reached a good target dose of 200–300 mg a day. Usually I will go up to 300 mg if they can tolerate it, and if in 4–6 weeks they haven’t improved, then it’s probably not going to work.
CATR: We sometimes hear about the use of these meds for people who have not yet developed a full AUD.
Dr. Arias: Right. There’s evidence that you can consider medications for people who drink too much but haven’t yet developed a full-blown AUD. And naltrexone can also be used in a targeted “as needed” way to prevent binge drinking when a patient is going to a certain event, such as a wedding, and is concerned about having a binge. The patient would take the naltrexone a couple of hours ahead of the event.
CATR: Let’s switch gears a bit and talk about the role of psychotherapy. The depression analogy comes up: We know that cognitive behavioral therapy (CBT) works, as do meds, but the combination may be better than either one alone. Is that true for AUD?
Dr. Arias: It’s not clear that it’s true for AUD. The literature supports the use of medications as well as certain psychotherapies as efficacious treatments; however, it’s not clear that adding psychotherapy to medications improves outcomes above medication by itself. Clinically, it pays to have a patient-centered approach and think about what’s going on with your patient’s specific case. There may be some advantages to therapy that the patient isn’t necessarily going to get with the medication, and vice versa.
CATR: In terms of outcomes, we used to think of abstinence. How should we think of outcomes nowadays?
Dr. Arias: For a long time this has been controversial, but recently there has been work that clearly frames reduction in drinking as a desired and sufficient outcome. There are some patients, usually because of the severity of their AUD or their comorbidities, who have very little control once they resume drinking. So, for some people there is reason to get them to try to be totally abstinent. But for most people, insisting on abstinence is probably just going to drive them out of treatment and break the therapeutic alliance.
CATR: So, reducing drinking is a reasonable outcome for most patients.
Dr. Arias: Exactly. There is a recent analysis looking at the World Health Organization’s drinking risk categories, and it shows that reducing a person’s risk category by at least 1 or preferably 2 levels is associated with much better overall outcomes (Witkiewitz K et al, Alcohol Clin Exp Res 2017;41(1):179–186). That may mean some people are still drinking a couple of times a week, maybe even drinking heavily on some days. But if they’ve substantially reduced their drinking, their health will be much improved. And that is concordant with a previous analysis using traditional abstinence and no heavy drinking outcomes, where it was shown that, while no heavy drinking is the best, there’s not a huge difference between heavy drinking occasionally and no heavy drinking.
CATR: We still have this idea that the first step is doing a detox. But we now know that most people go back to drinking. Is it worth recommending detox if we are rethinking outcomes in terms of reduction in drinking?
Dr. Arias: I don’t think we should give up detoxing entirely, but I think there may be people where insisting on detox first isn’t necessary. And since we now have at least one medication like topiramate that probably works well even if people are regularly drinking heavily and have mild withdrawal, we may be able to skip detox in some of those people. What I find is that clinically, there’s a certain point where people who drink heavily have induced a state that they really can’t safely go a day without drinking. So, I think we should shift toward assessing the severity of withdrawal and stratifying risk and the need for medically supervised detox. There are now some valid instruments that may help with the task, such as the Prediction of Alcohol Withdrawal Severity Scale (PAWSS) (Maldonado JR et al, Alcohol and Alcoholism 2015;50(5):509–518).
CATR: Thank you for your time, Dr. Arias.



Recommended


