
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
‘Why’d you give him Jailhouse Coke?’
A guard leans in and asks while you’re reviewing med orders on the correctional unit.
You glance at the chart. Bupropion 150 mg. That’s it.
But in here, that’s not “bupropion.”
It’s contraband. Currency. A known favorite on the prison barter circuit.
We don’t learn this in residency.
Most of us never hear that psychiatric meds come with street value behind bars and their own underground language.
A recent piece by Joshua Sonkiss, MD in The Carlat Hospital Psychiatry Report pulls back the curtain on what clinicians outside the correctional system rarely see:
The slang. The misuse. The way treatment gets reframed through a survival lens.
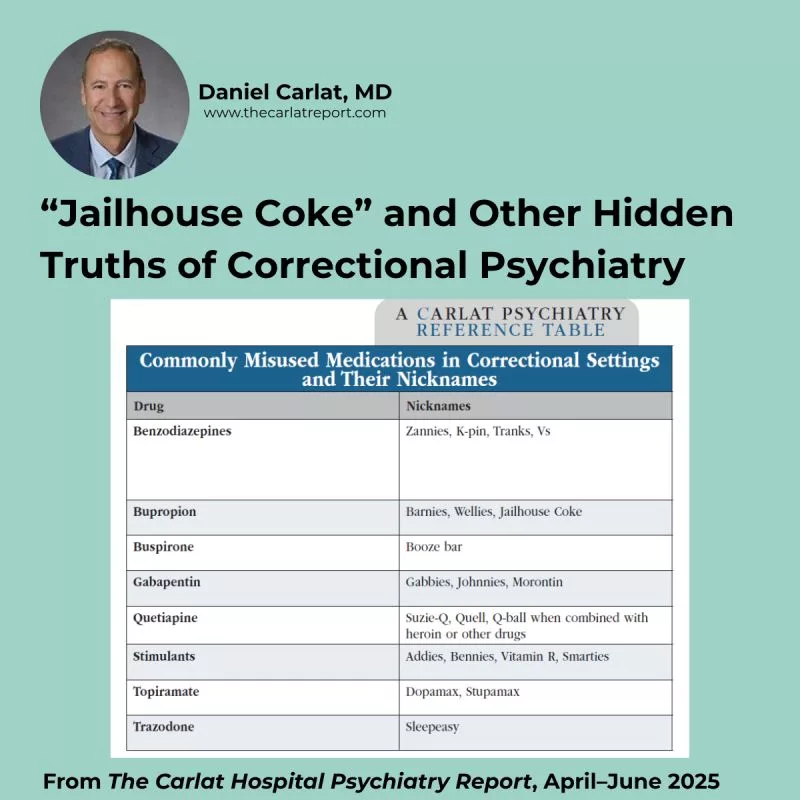
Here’s a sample of what patients and staff are actually calling these meds:
→ Bupropion → Barnies, Wellies, Jailhouse Coke
→ Gabapentin → Gabbies, Johnnies, Morontin
→ Quetiapine → Suzie-Q, Quell, Q-ball (when mixed with opioids)
→ Buspirone → Booze bar
→ Trazodone → Sleepeasy
→ Topiramate → Dopamax, Stupamax
→ Stimulants → Addies, Bennies, Vitamin R, Smarties
→ Benzos → Zannies, K-pins, Tranks, Vs
These aren’t just nicknames. They’re clues into behavior on the unit, potential for diversion, and patterns of misuse that don’t show up in the chart.
That’s why Sonkiss recommends a more adaptive prescribing approach:
→ Prioritize meds with lower street value
→ Ask officers about behavior on the unit
→ always weigh the clinical need against the risk of diversion.
This kind of psychiatry doesn’t show up in guidelines. But it shapes the safety of your unit. The effectiveness of your treatment. The trust between you and the patient.
We included the full table and recommendations in the April/May/June issue of CHPR.
It’s worth bookmarking if you ever rotate through inpatient, forensic, or correctional settings.
What about you?
Have you come across street names or diversion patterns that surprised you?
What’s shaped your prescribing in high-risk or high-surveillance settings?
Join the conversation on LinkedIn with Dr. Carlat
Related Articles
- Identifying and Treating Substance Use in Correctional Settings Author: Joshua Sonkiss, MD
- Psych Meds That Cause Weight Loss? Yes, They Exist. Author: Chris Aiken, MD
- Cobenfy: A New Antipsychotic Author: Chris Aiken, MD
- Weight Changes and Antidepressants: What to Tell Patients Author: Dominic Le, MD
Try The New AskCarlat AI

Recommended


