
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
Comparing Cholinesterase Inhibitors
If you were in TCR's editorial offices, surrounded by boxes of articles about acetylcholinesterase inhibitors (AChEI’s), you would quickly develop a sinking sensation. Not because the articles are so boring (though, in fact, they are); rather, because the pharmaceutical hype-sters are back on parade once again.
As with the SSRIs and the second generation antipsychotics, in which there are also several members of a class of meds, in the AChEI world there is intense jockeying for position, there are hired guns and pseudo-pharmacological advantages. Caveat emptor!
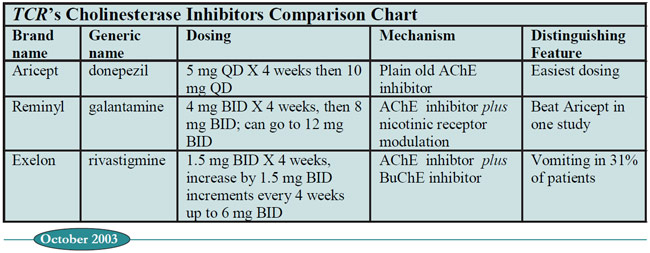
In this article, TCR compares the big three: Aricept, Reminyl, and Exelon. Sorry, Cognex (tacrine), but you don't make the cut. While you were the first to be approved in 1993, your bad habits of causing hepatotoxicity and bradycardia relegate you to a last-line bystander in this discussion.
Let's begin with names. TCR has developed mnemonics for associating the brand with the generic names of these compounds. Aricept is donepezil (the first letters juxtaposed are "AD" for Alzheimer's Disease); Reminyl is galantamine (the drug helps you to "Remember a big gala"); Exelon is rivastigmine ("Ex(c)el on a river of memory"). Take them or leave them!
All these drugs have been subjected to rigorous placebo-controlled trials. Three different outcomes are often examined: cognitive functioning, ADLs, and "behavioral symptoms," a somewhat misleading term that includes depression and delusions as well as the truly behavioral problems like agitation and wandering.
Just to give you a sense of the methodology used, we'll look at a representative study, one published in 2000 in Neurology comparing Reminyl with placebo (1). For inclusion, patients had to meet standard criteria for Alzheimers Dementia (AD), and their impairment could be no worse than "mild to moderate", that is, a Folstein Mini Mental State Exam (MMSE) score of 11-24; the average MMSE score in this study was 19. About 60% of patients were males, and the average age was about 75.
Patients were randomized to one of three treatment groups: placebo, moderate- dose Reminyl, or high-dose Reminyl. They were assessed periodically throughout the study with a well-loved measure of cognition in this research world: the ADAS-cog. It's confusingly scored, because a higher score means you're worse off, which is exactly the opposite of the MMSE.
Table: TCR’s Cholinesterase Inhibitors Comparison Chart
The results were typical for what is reported for all AChEIs: The medication triggered a small cognitive boost within the first couple of months, which gradually petered away until cognitive functioning was at pre-drug baseline by the end of year one. By contrast, patients on placebo were already well below their cognitive baseline at the 6 month mark, with ADAS-cog scores a full 4 points above the Reminyl group, and 2 points above their baseline (yes, above--I told you the ADAS-cog was confusing!).
The problem was a high drop-out rate due to side effects (primarily G.I.), in the 20-30% range depending on the dose of reminyl, vs. only 8% drop-out on placebo. This type of data, not unique to Reminyl, is what drives the recommendations for a very gradual dose titration schedules for all AChEIs, and studies that have incorporated these schedules have reported much lower drop-out rates.
The bottom-line is that all AChEIs work for AD; in addition, each of the big three now sports convincing data for efficacy in vascular dementia as well.
What happens when patients stop taking their AChEIs? Bad things. A report in the Archives of Neurology compared two ultra-long term studies of Aricept (lasting about 3 years), both of which started as standard placebo-controlled trials. In one study, after 6 months of Aricept treatment, patients were switched to placebo for 6 weeks before being allowed to resume Aricept in an open label extension of the study. Cognitive scores plummeted in these patients, right down to the lowly level of those who had been on placebo since day one! And even when these patients were "rescued" with open-label Aricept, cognitive decline continued, with no real respite for the weary. This effect also occurred in the group that was more mercifully washed out for only 3 weeks, but it was not nearly as dramatic. The moral of this story? Once a patient is on an AChEI, don't let them interrupt it, come hell or high water.
Now, onto the pharmaceutical gamesmanship section of our article. Do the so-called pharmacological distinctions between the drugs hold up under TCR's magnifying glass?
TCR VERDICT: Aricept’s Easiest; Reminyl Might be Better
1. Raskind MA, Peskind ER, Wessel T. Galantamine in AD: A 6-month randomized, placebo-controlled trial with a 6-month extension. Neurology 2000;54:2261-2268.
2. Doody RS, Geldmacher DS, Gordon B. Open-label, multicenter, phase 3 extension study of the safety and efficacy of donepezil in patients with Alzheimers Disease. Arch Neurol. 2001;58:427-433
3. Wilkinson DG, Passmore AP, Bullock R. A Multinational, randomized, 12-week, comparative study of donepezil and rivastigmine in patients with mild to moderate Alzheimers Disease. Int J Clin Pract 2002; 56:441-446.
4. Wilcock G, Howe I, Coles H. A long-term comparison of galantamine and donepezil in the treatment of Alzheimer’s Disease. Drugs Aging 2003; 20(10):777-789.
5. Package insert, rivastigmine.
General PsychiatryAs with the SSRIs and the second generation antipsychotics, in which there are also several members of a class of meds, in the AChEI world there is intense jockeying for position, there are hired guns and pseudo-pharmacological advantages. Caveat emptor!
In this article, TCR compares the big three: Aricept, Reminyl, and Exelon. Sorry, Cognex (tacrine), but you don't make the cut. While you were the first to be approved in 1993, your bad habits of causing hepatotoxicity and bradycardia relegate you to a last-line bystander in this discussion.
Are the “pharmacological distinctions” relevant, or marketing ploys?
Let's begin with names. TCR has developed mnemonics for associating the brand with the generic names of these compounds. Aricept is donepezil (the first letters juxtaposed are "AD" for Alzheimer's Disease); Reminyl is galantamine (the drug helps you to "Remember a big gala"); Exelon is rivastigmine ("Ex(c)el on a river of memory"). Take them or leave them!
All these drugs have been subjected to rigorous placebo-controlled trials. Three different outcomes are often examined: cognitive functioning, ADLs, and "behavioral symptoms," a somewhat misleading term that includes depression and delusions as well as the truly behavioral problems like agitation and wandering.
Just to give you a sense of the methodology used, we'll look at a representative study, one published in 2000 in Neurology comparing Reminyl with placebo (1). For inclusion, patients had to meet standard criteria for Alzheimers Dementia (AD), and their impairment could be no worse than "mild to moderate", that is, a Folstein Mini Mental State Exam (MMSE) score of 11-24; the average MMSE score in this study was 19. About 60% of patients were males, and the average age was about 75.
Patients were randomized to one of three treatment groups: placebo, moderate- dose Reminyl, or high-dose Reminyl. They were assessed periodically throughout the study with a well-loved measure of cognition in this research world: the ADAS-cog. It's confusingly scored, because a higher score means you're worse off, which is exactly the opposite of the MMSE.
Table: TCR’s Cholinesterase Inhibitors Comparison Chart
The results were typical for what is reported for all AChEIs: The medication triggered a small cognitive boost within the first couple of months, which gradually petered away until cognitive functioning was at pre-drug baseline by the end of year one. By contrast, patients on placebo were already well below their cognitive baseline at the 6 month mark, with ADAS-cog scores a full 4 points above the Reminyl group, and 2 points above their baseline (yes, above--I told you the ADAS-cog was confusing!).
The problem was a high drop-out rate due to side effects (primarily G.I.), in the 20-30% range depending on the dose of reminyl, vs. only 8% drop-out on placebo. This type of data, not unique to Reminyl, is what drives the recommendations for a very gradual dose titration schedules for all AChEIs, and studies that have incorporated these schedules have reported much lower drop-out rates.
The bottom-line is that all AChEIs work for AD; in addition, each of the big three now sports convincing data for efficacy in vascular dementia as well.
What happens when patients stop taking their AChEIs? Bad things. A report in the Archives of Neurology compared two ultra-long term studies of Aricept (lasting about 3 years), both of which started as standard placebo-controlled trials. In one study, after 6 months of Aricept treatment, patients were switched to placebo for 6 weeks before being allowed to resume Aricept in an open label extension of the study. Cognitive scores plummeted in these patients, right down to the lowly level of those who had been on placebo since day one! And even when these patients were "rescued" with open-label Aricept, cognitive decline continued, with no real respite for the weary. This effect also occurred in the group that was more mercifully washed out for only 3 weeks, but it was not nearly as dramatic. The moral of this story? Once a patient is on an AChEI, don't let them interrupt it, come hell or high water.
Now, onto the pharmaceutical gamesmanship section of our article. Do the so-called pharmacological distinctions between the drugs hold up under TCR's magnifying glass?
-
Do nicotinic receptors matter? Janssen certainly hopes they do. Reminyl modulates presynaptic nicotinic receptors, which causes cholinergic neurons to churn out ever more acetylcholine (ACh), with the hoped for result that your patient's memory improves.
And there is actually some evidence in support of this point. A multi-center study conducted in the U.K. and funded by Janssen compared 94 AD patients on Reminyl with 88 patients on Aricept. (4) After one year of treatment, Reminyl patients scored about 1.5 points higher on the MMSE than the Aricept patients. The catch? This study was neither placebo-controlled nor double-blinded. Why is this important? Because participating doctors knew which drug they were prescribing, and may have raised patients’ expectations with doctorly statements like: “Mr. Jones, we’re going to be putting you on the newest and most powerful memory drug available--Reminyl!” Never underestimate the power of suggestion.
- Does butyrylcholinesterase matter? BuCholE does exactly what ACholE does, namely, hydrolyzes and therefore inactivates acetylcholine. Exelon inhibits both BuChE and AChE, potentially making it more potent at revving up the cholinergic neurons. The problem is that most of the body’s BuChE lives in the GI tract, and its inhibition probably explains why Exelon causes nausea in 47% of patients and frank vomiting in an astonishing 31% (5). At this point, it appears that if BuCholE matters at all, it matters in a bad way for Novartis-worse tolerability than its competitors.
TCR VERDICT: Aricept’s Easiest; Reminyl Might be Better
1. Raskind MA, Peskind ER, Wessel T. Galantamine in AD: A 6-month randomized, placebo-controlled trial with a 6-month extension. Neurology 2000;54:2261-2268.
2. Doody RS, Geldmacher DS, Gordon B. Open-label, multicenter, phase 3 extension study of the safety and efficacy of donepezil in patients with Alzheimers Disease. Arch Neurol. 2001;58:427-433
3. Wilkinson DG, Passmore AP, Bullock R. A Multinational, randomized, 12-week, comparative study of donepezil and rivastigmine in patients with mild to moderate Alzheimers Disease. Int J Clin Pract 2002; 56:441-446.
4. Wilcock G, Howe I, Coles H. A long-term comparison of galantamine and donepezil in the treatment of Alzheimer’s Disease. Drugs Aging 2003; 20(10):777-789.
5. Package insert, rivastigmine.



Recommended


