
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
When AA Is Not the Answer: SMART Recovery and Other 12-Step Alternatives
Doctor: You might attend an AA meeting, if you’ve never been. They’re widely available, which makes it easy to find one nearby.
Patient: I agree I drink too much, but I don’t like all that “higher-power” stuff I’ve heard about AA meetings. I don’t think they would help me.
Doctor: Understood. No approach works for everyone. Fortunately, there are other groups, like SMART Recovery, that have similar goals—to help you overcome a drinking problem—but use different methods.
Patient: Really? Where can I learn more about them?
12-step groups: Why they’re not for everyone
Everyone knows about Alcoholics Anonymous (AA), the original 12-step group. There are more than 60,000 weekly AA meetings in the U.S. alone, and even more if we include Narcotics Anonymous (NA) and other 12-step groups (http://www.aa.org/assets/en_US/smf-53_en.pdf). What’s more, the AA model has become the foundation of most U.S. treatment paradigms. Despite this near-monopoly, however, many patients object to some of the most basic tenets of 12-step groups. In my experience, the common reasons patients balk at these groups can be found in the first three AA steps:
For many who are uncomfortable with quasi-religious AA practices such as prayer and meditation, or who identify as atheist or agnostic, the spiritual aspect of 12-step groups can be off-putting. Others do not believe that accepting a sense of powerlessness is a prerequisite to sobriety. Fortunately, patients in recovery have alternatives to choose from if they’d prefer not to attend a 12-step group. In this article, I will review the most popular one, SMART Recovery, as well as touch upon other recovery and mutual-help organizations in a separate box.
SMART Recovery
SMART Recovery (Self Management And Recovery Training), an international nonprofit founded in 1994, is the most widely available of the non-12-step groups. It has about 1,000 weekly meetings in the U.S., and about 2,000 worldwide. SMART meetings discuss any addictive behavior, whether it involves substances, activities like gambling or video games, or pornography. For patients who can’t find a local meeting, the group has a strong online presence, with daily virtual meetings in addition to a message board and 24/7 chatroom.
What are the basic elements of SMART Recovery? Perhaps most significantly, in contrast to AA’s emphasis on the need to yield to a higher power, SMART emphasizes self-empowerment (Horvath AT and Yeterian J, Journal Groups Addiction & Recovery 2012;7(2–4):102–117). This emphasis also means that SMART Recovery does not include a sponsorship system.
The SMART Recovery 4-Point Program®
The approach uses a 4-point program that addresses the following:
SMART meetings teach patients “tools of recovery” that are used to achieve each of the points. These tools are both therapy frameworks and actual worksheets, and they are drawn from the CBT (cognitive behavioral therapy) and MI (motivational interviewing) literature. They include the following:
Building and maintaining motivation
Participants weigh what’s positive about drinking against the long-term consequences. This allows them to assess whether, on balance, drinking is actually “worth it.” A meeting leader can help participants set up their balance sheet. That allows them to articulate, for instance, that on the positive side drinking makes them feel more relaxed and removes them from anxiety-provoking situations. On the negative side, however, the substance may have cost them important relationships or even jobs. Writing these items out on a balance sheet helps people assess the true cost of their addiction.
Coping with urges
Participants receive rational emotive behavior therapy guidance on how to avoid abusing substances in real time, meaning when they are in a place that triggers the urge to use. Rational, intellectual responses to excuses for using—in other words, responses in the moment—are encouraged. For example, on the way home a person is thinking about stopping into a bar or liquor store as a way of “making up for” a bad day at work. But using SMART techniques, the person thinks it through and is able to mentally say, “Alcohol doesn’t make up for a hard day at the office. The two are not related, and in fact, alcohol can only make things worse. I could end up coming in groggy tomorrow and not on top of my game when things are already thorny.”
Managing thoughts, feelings, and behaviors
Participants are taught to carefully examine their mindset so that they can prevent negative feelings from overwhelming them. Perhaps a participant takes offense easily, overreacting to slights and feeling bad as a result. Once the person realizes this is a pattern, it’s possible through SMART techniques to prevent downward-spiraling thoughts and feelings—the same feelings that could easily lead to substance use.
Living a balanced life
Lifestyle balance is an important aspect of finding alternatives to substance use. Pursuing a hobby or other pastime, making better connections with those in one’s life, meeting new people—all of these activities can lead to long-lasting recovery.
These are the underpinnings, but how do they play out in a SMART Recovery meeting?
What a SMART Recovery meeting actually feels like
Perhaps the most striking aspect of a SMART meeting is the “cross-talk.” In traditional 12-step meetings, participants take turns sharing aspects of their recovery stories. Each story is typically told without reference to any other story.
SMART meetings, by contrast, are active discussions in which all may engage freely. The meeting guidelines include staying focused on recovery, not talking too long or disrespectfully, and not giving advice, although suggestions are welcome. What’s the difference between advice and suggestion? Often, it’s the speaker’s tone. “You need to be on opioid substitution” is advice. “Have you considered the possibility of opioid substitution?” is a suggestion.
The meeting agenda typically includes a welcome, a brief check-in around the circle, establishing the topics of discussion for that meeting, a discussion period (the longest portion of the 60- or 90-minute meeting), passing the hat for donations and making announcements, and a check-out. No one is required to participate or use any particular language, such as calling oneself an “addict” or “alcoholic”—terms SMART discourages (but accepts if a participant wants to use them). These words are discouraged because SMART Recovery participants may see their behavior on a continuum rather than as an all-or-nothing condition. Also, if a participant adopts a term like “alcoholic,” that person might feel labeled for life rather than being able to say at some point, “I had a problem, and now it is in the past.”
In a similar vein, SMART meetings are noteworthy for their relative lack of insistence about how participants should think about their problem in general. Participants are free to believe addiction is a disease or not (some see it simply as a bad habit), to believe in a higher power or not, and to decide which (if any!) substances to abstain from. The SMART slogan, “Discover the Power of Choice,” captures this personalized aspect. AA, by contrast, relies on a shared understanding that alcoholism, like diabetes, is a disease that can be treated but never cured.
That said, for some participants, attending both 12-step and SMART meetings appears to be helpful (http://www.rehabs.com/pro-talk-articles/the-dual-citizenship-phenomenon-2/), even though the philosophies of the two can sometimes be at odds. People will often say, “I go to SMART for tools and AA for fellowship.” AA does fellowship very well, and from my observations, shared bonding does more for a lot of followers than the 12 steps themselves or the spiritual component.
In the SMART program, absolute “recovery” is not necessarily the goal. While some participants may choose to embrace abstinence, others may decide to moderate their drinking. SMART tends to have more flexibility in the recovery method than AA, which is focused on complete abstinence.
While the focus of a SMART meeting is on “stopping,” it’s important to remember that stopping doesn’t necessarily mean abstaining. Participants can decide whether to stop before the first drink, for instance, or after the third. They can also decide to stop their opiate use but continue using cannabis. Although some participants may be tempted to emphasize how they are going to be successful moderating, an effective meeting leader will interrupt and say, “You are here because you had trouble stopping. No one has trouble using—you don’t need any help with using! Let’s stay focused on how to stop, and you can decide when and where to employ those skills.”
People who attend SMART Recovery meetings are not encouraged to go for life, as some members of AA like to do. Instead, they are encouraged to go until they solve their problem.
Evidence for the effectiveness of SMART Recovery
Evidence about SMART Recovery’s effectiveness is in the early stages but promising. In February of this year, the first systematic review article was published (Beck A et al, Psychol Addict Behav 2017;31(1):1–20. doi:10.1037/adb0000237), covering 12 studies. The overall conclusions are that SMART is helpful for specific populations (alcohol, corrections, and comorbidity thus far) and that SMART may be more time-efficient than other approaches. The largest study, with 5,764 subjects in the Australian prison system, found that SMART improved outcomes beyond standard programming if there was a sufficient dose of it (20 hours). Another study involving 50 day hospital patients found that the SMART Recovery approach generally worked as well as 12-step care, as measured by the Addiction Severity Index, a quality of life measure, and urinalysis results.
Interestingly, one study comparing participants in various mutual-help groups found that improvement occurred in all of them, despite their radically different approaches. However, participants whose beliefs were more closely matched to the group had better outcomes. Participants who scored high on religiosity, for instance, had better participation in AA.
Bottom-line recommendations
Doctor: How did those recovery meetings go?
Patient: Thanks for the information that several types of recovery meetings exist. I went to two AA meetings. I didn’t like the first one that much, but I wanted to give it a fair chance, so I went to a different one. I still didn’t like it, but I can see how it would be helpful for some people. The SMART meeting, though, I liked right away. It was conversational, and by the end I was participating too. I picked up a couple of ideas, and even bought their handbook, which I want to study. In SMART, they actively work on how to think differently.
Doctor: How so?
Patient: Before, I was convinced that if a thought popped into my head, I was stuck with it. Now, I realize it’s okay for me to examine a thought—or a feeling—and see if it really squares with what’s going on in my life. It’s okay for me to challenge something in my head that isn’t working for me.
Doctor: Sounds like a reminder we could all use!
CATR Verdict: 12-step groups like AA will continue to be an important resource. However, 12-step alternatives like SMART Recovery are gaining acceptance—and scientific support—in an increasingly secular world. For patients who find they can’t relate to the 12 steps, such alternatives are worth recommending.
Addiction TreatmentPatient: I agree I drink too much, but I don’t like all that “higher-power” stuff I’ve heard about AA meetings. I don’t think they would help me.
Doctor: Understood. No approach works for everyone. Fortunately, there are other groups, like SMART Recovery, that have similar goals—to help you overcome a drinking problem—but use different methods.
Patient: Really? Where can I learn more about them?
12-step groups: Why they’re not for everyone
Everyone knows about Alcoholics Anonymous (AA), the original 12-step group. There are more than 60,000 weekly AA meetings in the U.S. alone, and even more if we include Narcotics Anonymous (NA) and other 12-step groups (http://www.aa.org/assets/en_US/smf-53_en.pdf). What’s more, the AA model has become the foundation of most U.S. treatment paradigms. Despite this near-monopoly, however, many patients object to some of the most basic tenets of 12-step groups. In my experience, the common reasons patients balk at these groups can be found in the first three AA steps:
- We admitted we were powerless over alcohol—that our lives had become unmanageable.
- Came to believe that a Power greater than ourselves could restore us to sanity.
- Made a decision to turn our will and our lives over to God as we understood him (Alcoholics Anonymous (2001). Alcoholics Anonymous, 4th ed. New York: A.A. World Services).
For many who are uncomfortable with quasi-religious AA practices such as prayer and meditation, or who identify as atheist or agnostic, the spiritual aspect of 12-step groups can be off-putting. Others do not believe that accepting a sense of powerlessness is a prerequisite to sobriety. Fortunately, patients in recovery have alternatives to choose from if they’d prefer not to attend a 12-step group. In this article, I will review the most popular one, SMART Recovery, as well as touch upon other recovery and mutual-help organizations in a separate box.
SMART Recovery
SMART Recovery (Self Management And Recovery Training), an international nonprofit founded in 1994, is the most widely available of the non-12-step groups. It has about 1,000 weekly meetings in the U.S., and about 2,000 worldwide. SMART meetings discuss any addictive behavior, whether it involves substances, activities like gambling or video games, or pornography. For patients who can’t find a local meeting, the group has a strong online presence, with daily virtual meetings in addition to a message board and 24/7 chatroom.
What are the basic elements of SMART Recovery? Perhaps most significantly, in contrast to AA’s emphasis on the need to yield to a higher power, SMART emphasizes self-empowerment (Horvath AT and Yeterian J, Journal Groups Addiction & Recovery 2012;7(2–4):102–117). This emphasis also means that SMART Recovery does not include a sponsorship system.
The SMART Recovery 4-Point Program®
The approach uses a 4-point program that addresses the following:
- Building and maintaining motivation
- Coping with urges
- Managing thoughts, feelings, and behaviors
- Living a balanced life
SMART meetings teach patients “tools of recovery” that are used to achieve each of the points. These tools are both therapy frameworks and actual worksheets, and they are drawn from the CBT (cognitive behavioral therapy) and MI (motivational interviewing) literature. They include the following:
- Stages of change and a change plan worksheet
- Cost/benefit analysis (decision-making worksheet)
- ABCs of REBT (rational emotive behavior therapy) for urge coping
- Hierarchy of values
- Role-playing and rehearsing
- USA (Unconditional Self-Acceptance)
- The length of this article precludes giving examples of each tool in the context of achieving the 4 Points, but some key examples follow.
Building and maintaining motivation
Participants weigh what’s positive about drinking against the long-term consequences. This allows them to assess whether, on balance, drinking is actually “worth it.” A meeting leader can help participants set up their balance sheet. That allows them to articulate, for instance, that on the positive side drinking makes them feel more relaxed and removes them from anxiety-provoking situations. On the negative side, however, the substance may have cost them important relationships or even jobs. Writing these items out on a balance sheet helps people assess the true cost of their addiction.
Coping with urges
Participants receive rational emotive behavior therapy guidance on how to avoid abusing substances in real time, meaning when they are in a place that triggers the urge to use. Rational, intellectual responses to excuses for using—in other words, responses in the moment—are encouraged. For example, on the way home a person is thinking about stopping into a bar or liquor store as a way of “making up for” a bad day at work. But using SMART techniques, the person thinks it through and is able to mentally say, “Alcohol doesn’t make up for a hard day at the office. The two are not related, and in fact, alcohol can only make things worse. I could end up coming in groggy tomorrow and not on top of my game when things are already thorny.”
Managing thoughts, feelings, and behaviors
Participants are taught to carefully examine their mindset so that they can prevent negative feelings from overwhelming them. Perhaps a participant takes offense easily, overreacting to slights and feeling bad as a result. Once the person realizes this is a pattern, it’s possible through SMART techniques to prevent downward-spiraling thoughts and feelings—the same feelings that could easily lead to substance use.
Living a balanced life
Lifestyle balance is an important aspect of finding alternatives to substance use. Pursuing a hobby or other pastime, making better connections with those in one’s life, meeting new people—all of these activities can lead to long-lasting recovery.
These are the underpinnings, but how do they play out in a SMART Recovery meeting?
What a SMART Recovery meeting actually feels like
Perhaps the most striking aspect of a SMART meeting is the “cross-talk.” In traditional 12-step meetings, participants take turns sharing aspects of their recovery stories. Each story is typically told without reference to any other story.
SMART meetings, by contrast, are active discussions in which all may engage freely. The meeting guidelines include staying focused on recovery, not talking too long or disrespectfully, and not giving advice, although suggestions are welcome. What’s the difference between advice and suggestion? Often, it’s the speaker’s tone. “You need to be on opioid substitution” is advice. “Have you considered the possibility of opioid substitution?” is a suggestion.
The meeting agenda typically includes a welcome, a brief check-in around the circle, establishing the topics of discussion for that meeting, a discussion period (the longest portion of the 60- or 90-minute meeting), passing the hat for donations and making announcements, and a check-out. No one is required to participate or use any particular language, such as calling oneself an “addict” or “alcoholic”—terms SMART discourages (but accepts if a participant wants to use them). These words are discouraged because SMART Recovery participants may see their behavior on a continuum rather than as an all-or-nothing condition. Also, if a participant adopts a term like “alcoholic,” that person might feel labeled for life rather than being able to say at some point, “I had a problem, and now it is in the past.”
In a similar vein, SMART meetings are noteworthy for their relative lack of insistence about how participants should think about their problem in general. Participants are free to believe addiction is a disease or not (some see it simply as a bad habit), to believe in a higher power or not, and to decide which (if any!) substances to abstain from. The SMART slogan, “Discover the Power of Choice,” captures this personalized aspect. AA, by contrast, relies on a shared understanding that alcoholism, like diabetes, is a disease that can be treated but never cured.
That said, for some participants, attending both 12-step and SMART meetings appears to be helpful (http://www.rehabs.com/pro-talk-articles/the-dual-citizenship-phenomenon-2/), even though the philosophies of the two can sometimes be at odds. People will often say, “I go to SMART for tools and AA for fellowship.” AA does fellowship very well, and from my observations, shared bonding does more for a lot of followers than the 12 steps themselves or the spiritual component.
In the SMART program, absolute “recovery” is not necessarily the goal. While some participants may choose to embrace abstinence, others may decide to moderate their drinking. SMART tends to have more flexibility in the recovery method than AA, which is focused on complete abstinence.
While the focus of a SMART meeting is on “stopping,” it’s important to remember that stopping doesn’t necessarily mean abstaining. Participants can decide whether to stop before the first drink, for instance, or after the third. They can also decide to stop their opiate use but continue using cannabis. Although some participants may be tempted to emphasize how they are going to be successful moderating, an effective meeting leader will interrupt and say, “You are here because you had trouble stopping. No one has trouble using—you don’t need any help with using! Let’s stay focused on how to stop, and you can decide when and where to employ those skills.”
People who attend SMART Recovery meetings are not encouraged to go for life, as some members of AA like to do. Instead, they are encouraged to go until they solve their problem.
Evidence for the effectiveness of SMART Recovery
Evidence about SMART Recovery’s effectiveness is in the early stages but promising. In February of this year, the first systematic review article was published (Beck A et al, Psychol Addict Behav 2017;31(1):1–20. doi:10.1037/adb0000237), covering 12 studies. The overall conclusions are that SMART is helpful for specific populations (alcohol, corrections, and comorbidity thus far) and that SMART may be more time-efficient than other approaches. The largest study, with 5,764 subjects in the Australian prison system, found that SMART improved outcomes beyond standard programming if there was a sufficient dose of it (20 hours). Another study involving 50 day hospital patients found that the SMART Recovery approach generally worked as well as 12-step care, as measured by the Addiction Severity Index, a quality of life measure, and urinalysis results.
Interestingly, one study comparing participants in various mutual-help groups found that improvement occurred in all of them, despite their radically different approaches. However, participants whose beliefs were more closely matched to the group had better outcomes. Participants who scored high on religiosity, for instance, had better participation in AA.
Bottom-line recommendations
- If 12-step groups are not acceptable to your patient, refer the patient to an alternative group, such as SMART Recovery. If there are no alternative groups locally, encourage exploration of online resources.
- Encourage your patient to be open-minded about 12-step groups, even if the patient has fundamental disagreements with them—it’s possible attendance may still be beneficial. The patient doesn’t need to accept every aspect of the 12-step approach. For many, simply joining a community of non-drinkers and non-users is the most effective aspect of a 12-step program, not the approach the program employs (Kelly JF et al, Drug Alcohol Depend 2013;129(1–2):151–157).
- If your patient refuses to attend a mutual-help group, encourage psychotherapy. Mutual-help groups are not essential to recovery. Psychotherapy is expensive and it does not provide a community support aspect, but it works for many. Some patients engage in both methods.
- Keep following up. The greatest virtue in addiction recovery, as in life, may be persistence. Most of these patients will ultimately recover or substantially improve, including the severe cases (U.S. Department of Health and Human Services, Office of the Surgeon General, 2016: 5–6). Even if none of the resources you propose are acceptable to the patient, place the problem back in the patient’s hands, and keep asking for progress reports.
Doctor: How did those recovery meetings go?
Patient: Thanks for the information that several types of recovery meetings exist. I went to two AA meetings. I didn’t like the first one that much, but I wanted to give it a fair chance, so I went to a different one. I still didn’t like it, but I can see how it would be helpful for some people. The SMART meeting, though, I liked right away. It was conversational, and by the end I was participating too. I picked up a couple of ideas, and even bought their handbook, which I want to study. In SMART, they actively work on how to think differently.
Doctor: How so?
Patient: Before, I was convinced that if a thought popped into my head, I was stuck with it. Now, I realize it’s okay for me to examine a thought—or a feeling—and see if it really squares with what’s going on in my life. It’s okay for me to challenge something in my head that isn’t working for me.
Doctor: Sounds like a reminder we could all use!
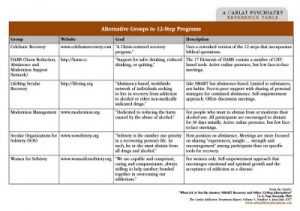
Table: Alternative Groups to 12-Step Programs
(Click here to view full-size PDF.)
CATR Verdict: 12-step groups like AA will continue to be an important resource. However, 12-step alternatives like SMART Recovery are gaining acceptance—and scientific support—in an increasingly secular world. For patients who find they can’t relate to the 12 steps, such alternatives are worth recommending.


Recommended


