
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.jpg?1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
Managing Pain: A Cognitive Behavioral Therapist’s Approach
As a clinical psychologist with a specialty in chronic pain management, I am often referred patients with both chronic pain and psychiatric issues. Many of these patients see a psychiatrist and a therapist, and are taking with both psychotropic and pain medications. The referral is often made because there is a sense that psychological issues are complicating the patient’s pain management.
In this article, I’ll describe how psychologists conceptualize the treatment of chronic pain and provide some tips for how you, as a busy prescriber, can leverage some of the successful techniques I use with my patients.
I’ll start by introducing a case of a veteran who is typical of my practice (I have altered the details to preserve confidentiality).
Martin C. is a 37-year-old U.S. veteran who was honorably discharged three years ago after four tours of duty in Iraq and Afghanistan. During his last tour, he sustained multiple injuries after an improvised explosive device detonated in close proximity to his Humvee. Three years later, he suffers from chronic low back pain and shoulder pain, and has been diagnosed with both PTSD and depression. He is taking milnacipran and prazosin for his psychiatric symptoms, and hydrocodone as needed for chronic pain. His referring psychiatrist says that Martin has partially responded to his meds but is still depressed and not very active. I am asked to help Martin learn some cognitive behavioral skills to manage his pain more effectively.
Cognitive behavioral therapy (CBT)
Most of you are probably familiar with basic cognitive behavioral therapy (CBT) concepts. As a reminder, CBT focuses on teaching people ways to identify and change counterproductive automatic thoughts and maladaptive behaviors, and to replace them with more adaptive ones. For example, a typical automatic thought in a patient with depression might be “I’m a failure.” In CBT, we help patients become aware of such cognitions, teach them to examine the evidence that supports the thought, and to generate alternative thoughts that are more balanced and adaptive. If therapy is successful, a patient will be able to recognize automatic thoughts as they occur, and counter them with more realistic thoughts. Over time, the adaptive thoughts become stronger and take the place of those that have been causing distress.
How does CBT work in pain management?
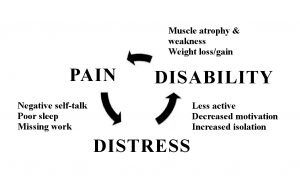
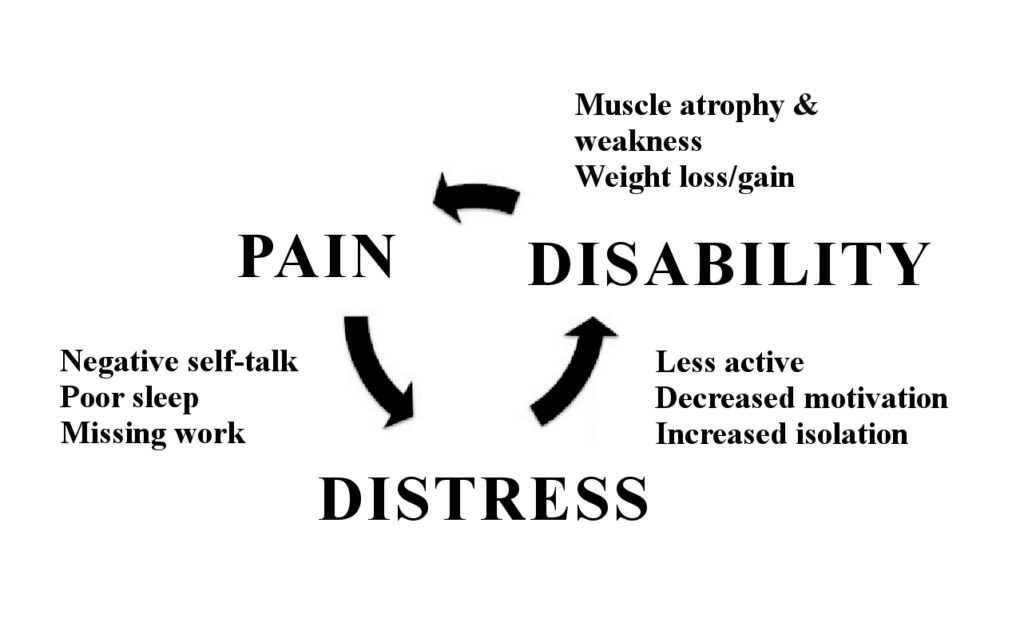
When I meet a new patient, I often start by taking out a sheet of paper and drawing the “Cycle of Pain,” which includes pain, distress, and disability (see figure below). The essence of this vicious cycle is that chronic pain can lead to negative automatic thoughts, insomnia, and isolation, all of which contribute to distress/depression.
Typical examples of maladaptive thoughts in pain patients include “I’m worthless to my family because I can’t work,” “I could have done so much with my life,” “This is never going to get better,” or “I’d better not be too active or I’m going to be in more pain.” Such thoughts lead not only to depression, but also to isolation and inactivity. Patients may isolate themselves to avoid others, in part because they get tired of hearing questions like, “Why aren’t you working? You look fine to me.” Less activity may lead to muscle atrophy and weight gain, both of which can aggravate the original pain condition. The decreased activity and deconditioning lead to more pain.
In my experience, patients with chronic pain will recognize this cycle and will be able to acknowledge that it has affected their lives and worsened their pain.
Evaluating pain
Returning to Martin, at our first meeting I conducted a typical comprehensive pain assessment assessment: I evaluated the location and quality of his pain, as well as his pain triggers, and took a standard psychiatric history. When I asked him about any strategies he had learned to cope with his pain, Martin responded, “I guess there’s really nothing I do but sit down, rest, and play video games to distract myself.” He used to enjoy fishing and photography, but he felt that his pain made those hobbies impossible to continue. He said he thought that life was passing him by. When I asked Martin, “Have you ever noticed a connection between your mood and pain?” he responded that he had, and that in particular the pain caused him to have a “short fuse” with everyone around him. He also realized that he had lost his motivation to take the steps necessary to return to college and develop a new career.
Cycle of Pain
Based on my assessment of Martin, there were several areas that were clear targets for intervention. First, Martin was depressed due to his tendency to engage in negative and catastrophic thinking about his future and his withdrawal from reinforcing activities. He needed to learn adaptive ways of addressing his negative thoughts, to get involved in activities that would bring happiness back into his life, and to make a plan to move forward with his educational interests. Second, Martin had a difficult time doing things at a slower pace. This is quite typical of people in the military, who are trained to not stop a job until it is complete. On a typical day he would spend hours playing Call of Duty; however, if he had a day when he was experiencing less pain, he would try to accomplish everything on his “to-do” list only to find himself in greater pain the next day.
Creating a treatment plan
Once I conduct an initial assessment, I work with the patient in coming up with a treatment plan. This typically involves the following elements:
Applying a treatment plan
Once I developed my case conceptualization, here’s how I proceeded with Martin’s therapy. In our first session, I made sure that Martin understood the connections between his thoughts, feelings, and behaviors and his pain. Unless patients agree with the treatment rationale, in my experience they often will not return.
Another activity I did with Martin, which I typically teach to my patients, is relaxation using diaphragm breathing. This technique serves two purposes: it teaches patients a useful skill right from the start of therapy, and it helps them to begin to notice how their body feels in reaction to their thoughts. This intervention by itself can be very powerful.
Martin and I set some overall goals for treatment, including resuming his hobbies and looking into colleges. The plan was to gradually reintroduce those activities into his life in a safe way. For example, although his pain made it difficult for him to fish from a boat, we brainstormed less demanding ways to fish, such as from a bridge or the shore.
In subsequent sessions, I taught him about cognitive restructuring. Over the ensuing sessions, he completed these types of homework sheets and was eventually able to restructure negative thoughts on his own. For example, Martin reported that he often told himself, “My life is ruined now; I can’t do anything,” which made him feel frustrated and depressed. Using a restructuring sheet, Martin wrote down this thought and the associated emotions. Under “evidence for the thought,” he wrote that his plans of having a military career were over, and he couldn’t engage in sports like he used to. In the category of “evidence against the thought,” he wrote that there are actually many things he can do, he has people who care about him, and he knows that he can learn new skills.
After reflecting on what he had written, Martin realized that there was little evidence to support his conviction that his life was “ruined.” Next, I urged Martin to write down a positive coping thought based on actual evidence; he wrote: “Although there are some career paths that I’m not going to be able to take, and I may have to do some things differently, I know I can learn new skills and find a new direction for myself. When one door closes, another one opens.” Martin commented that some of the thoughts he was having related to PTSD could also be challenged using restructuring.
In other sessions, we covered topics such as sleep hygiene, pleasant activity scheduling, and anger management. To discuss sleep hygiene, I typically use a patient education sheet, an example of which can be found on Pain-Resources. Pleasant activity scheduling is pretty much what it sounds like—we identified enjoyable activities that Martin could realistically perform and scheduled them into his week. Finally, anger management focused on helping him to identify thoughts that were contributing to anger, common triggers, and ways to be assertive but not aggressive.
Given his tendency to overdo it, Martin was taught to pace himself based on “time” and not “the job.” The example I often give to patients is, “Think of your favorite athletes—do they play the entire game nonstop or do they take breaks?” I asked Martin to think of himself as an athlete who wants to give the best performance possible, which resonated with him.
By the end of therapy, Martin had a much greater ability to challenge negative thoughts. Most of the ones that had been troubling him in the past were no longer an issue; in fact, he described them as “spam.” Martin was excited because he had selected a college and was enrolled in courses for the semester. While he had only managed to get his camera out a few times, he was fishing regularly and had made some new friends with the same interest. An important part of all of his progress was that he was pacing himself—he was thinking ahead and planning out what he needed to do in advance to set himself up for success. Martin still had chronic pain, and some days were tougher than others, but he was less depressed and more active, he knew how to talk to himself when he was in pain, and he was moving forward with his life.
Bottom line tips to use in your practice
While not all providers have access to a clinical psychologist with training in CBT for pain, there are several things that even busy prescribers can do to help patients.
For more information, see:
http://www.painpsych.com/
Otis, JD. Managing Chronic Pain: A Cognitive-Behavioral Therapy Approach, Therapist Guide. Treatments that Work Series. New York, NY: Oxford University Press; 2007.
Otis, JD. Managing Chronic Pain: A Cognitive-Behavioral Therapy Approach, Patient Workbook. Treatments that Work Series. New York, NY: Oxford University Press; 2007.
General PsychiatryIn this article, I’ll describe how psychologists conceptualize the treatment of chronic pain and provide some tips for how you, as a busy prescriber, can leverage some of the successful techniques I use with my patients.
I’ll start by introducing a case of a veteran who is typical of my practice (I have altered the details to preserve confidentiality).
Martin C. is a 37-year-old U.S. veteran who was honorably discharged three years ago after four tours of duty in Iraq and Afghanistan. During his last tour, he sustained multiple injuries after an improvised explosive device detonated in close proximity to his Humvee. Three years later, he suffers from chronic low back pain and shoulder pain, and has been diagnosed with both PTSD and depression. He is taking milnacipran and prazosin for his psychiatric symptoms, and hydrocodone as needed for chronic pain. His referring psychiatrist says that Martin has partially responded to his meds but is still depressed and not very active. I am asked to help Martin learn some cognitive behavioral skills to manage his pain more effectively.
Cognitive behavioral therapy (CBT)
Most of you are probably familiar with basic cognitive behavioral therapy (CBT) concepts. As a reminder, CBT focuses on teaching people ways to identify and change counterproductive automatic thoughts and maladaptive behaviors, and to replace them with more adaptive ones. For example, a typical automatic thought in a patient with depression might be “I’m a failure.” In CBT, we help patients become aware of such cognitions, teach them to examine the evidence that supports the thought, and to generate alternative thoughts that are more balanced and adaptive. If therapy is successful, a patient will be able to recognize automatic thoughts as they occur, and counter them with more realistic thoughts. Over time, the adaptive thoughts become stronger and take the place of those that have been causing distress.
How does CBT work in pain management?
When I meet a new patient, I often start by taking out a sheet of paper and drawing the “Cycle of Pain,” which includes pain, distress, and disability (see figure below). The essence of this vicious cycle is that chronic pain can lead to negative automatic thoughts, insomnia, and isolation, all of which contribute to distress/depression.
Typical examples of maladaptive thoughts in pain patients include “I’m worthless to my family because I can’t work,” “I could have done so much with my life,” “This is never going to get better,” or “I’d better not be too active or I’m going to be in more pain.” Such thoughts lead not only to depression, but also to isolation and inactivity. Patients may isolate themselves to avoid others, in part because they get tired of hearing questions like, “Why aren’t you working? You look fine to me.” Less activity may lead to muscle atrophy and weight gain, both of which can aggravate the original pain condition. The decreased activity and deconditioning lead to more pain.
In my experience, patients with chronic pain will recognize this cycle and will be able to acknowledge that it has affected their lives and worsened their pain.
Evaluating pain
Returning to Martin, at our first meeting I conducted a typical comprehensive pain assessment assessment: I evaluated the location and quality of his pain, as well as his pain triggers, and took a standard psychiatric history. When I asked him about any strategies he had learned to cope with his pain, Martin responded, “I guess there’s really nothing I do but sit down, rest, and play video games to distract myself.” He used to enjoy fishing and photography, but he felt that his pain made those hobbies impossible to continue. He said he thought that life was passing him by. When I asked Martin, “Have you ever noticed a connection between your mood and pain?” he responded that he had, and that in particular the pain caused him to have a “short fuse” with everyone around him. He also realized that he had lost his motivation to take the steps necessary to return to college and develop a new career.
Cycle of Pain
Based on my assessment of Martin, there were several areas that were clear targets for intervention. First, Martin was depressed due to his tendency to engage in negative and catastrophic thinking about his future and his withdrawal from reinforcing activities. He needed to learn adaptive ways of addressing his negative thoughts, to get involved in activities that would bring happiness back into his life, and to make a plan to move forward with his educational interests. Second, Martin had a difficult time doing things at a slower pace. This is quite typical of people in the military, who are trained to not stop a job until it is complete. On a typical day he would spend hours playing Call of Duty; however, if he had a day when he was experiencing less pain, he would try to accomplish everything on his “to-do” list only to find himself in greater pain the next day.
Creating a treatment plan
Once I conduct an initial assessment, I work with the patient in coming up with a treatment plan. This typically involves the following elements:
- Developing several overall goals for therapy and creating a strategy for goal achievement. This is done by setting small achievable goals each week that gradually move patients toward overall goal accomplishment.
- Teaching patients how to relax by noticing how they are breathing, how they are feeling, and what they are thinking. This is accomplished using diaphragmatic breathing, visual imagery, and progressive muscle relaxation.
- Replacing negative automatic thoughts with more realistic thoughts. This is also known as cognitive restructuring. My technique involves using a “restructuring sheet,” which is a page divided into several columns that require patients to write down their thoughts, feelings, evidence for and against a thought, and an alternative thought based on the actual evidence. Although these sheets initially require effort to complete, eventually they become unnecessary because patients learn to restructure thoughts in their heads.
Applying a treatment plan
Once I developed my case conceptualization, here’s how I proceeded with Martin’s therapy. In our first session, I made sure that Martin understood the connections between his thoughts, feelings, and behaviors and his pain. Unless patients agree with the treatment rationale, in my experience they often will not return.
Another activity I did with Martin, which I typically teach to my patients, is relaxation using diaphragm breathing. This technique serves two purposes: it teaches patients a useful skill right from the start of therapy, and it helps them to begin to notice how their body feels in reaction to their thoughts. This intervention by itself can be very powerful.
Martin and I set some overall goals for treatment, including resuming his hobbies and looking into colleges. The plan was to gradually reintroduce those activities into his life in a safe way. For example, although his pain made it difficult for him to fish from a boat, we brainstormed less demanding ways to fish, such as from a bridge or the shore.
In subsequent sessions, I taught him about cognitive restructuring. Over the ensuing sessions, he completed these types of homework sheets and was eventually able to restructure negative thoughts on his own. For example, Martin reported that he often told himself, “My life is ruined now; I can’t do anything,” which made him feel frustrated and depressed. Using a restructuring sheet, Martin wrote down this thought and the associated emotions. Under “evidence for the thought,” he wrote that his plans of having a military career were over, and he couldn’t engage in sports like he used to. In the category of “evidence against the thought,” he wrote that there are actually many things he can do, he has people who care about him, and he knows that he can learn new skills.
After reflecting on what he had written, Martin realized that there was little evidence to support his conviction that his life was “ruined.” Next, I urged Martin to write down a positive coping thought based on actual evidence; he wrote: “Although there are some career paths that I’m not going to be able to take, and I may have to do some things differently, I know I can learn new skills and find a new direction for myself. When one door closes, another one opens.” Martin commented that some of the thoughts he was having related to PTSD could also be challenged using restructuring.
In other sessions, we covered topics such as sleep hygiene, pleasant activity scheduling, and anger management. To discuss sleep hygiene, I typically use a patient education sheet, an example of which can be found on Pain-Resources. Pleasant activity scheduling is pretty much what it sounds like—we identified enjoyable activities that Martin could realistically perform and scheduled them into his week. Finally, anger management focused on helping him to identify thoughts that were contributing to anger, common triggers, and ways to be assertive but not aggressive.
Given his tendency to overdo it, Martin was taught to pace himself based on “time” and not “the job.” The example I often give to patients is, “Think of your favorite athletes—do they play the entire game nonstop or do they take breaks?” I asked Martin to think of himself as an athlete who wants to give the best performance possible, which resonated with him.
By the end of therapy, Martin had a much greater ability to challenge negative thoughts. Most of the ones that had been troubling him in the past were no longer an issue; in fact, he described them as “spam.” Martin was excited because he had selected a college and was enrolled in courses for the semester. While he had only managed to get his camera out a few times, he was fishing regularly and had made some new friends with the same interest. An important part of all of his progress was that he was pacing himself—he was thinking ahead and planning out what he needed to do in advance to set himself up for success. Martin still had chronic pain, and some days were tougher than others, but he was less depressed and more active, he knew how to talk to himself when he was in pain, and he was moving forward with his life.
Bottom line tips to use in your practice
While not all providers have access to a clinical psychologist with training in CBT for pain, there are several things that even busy prescribers can do to help patients.
- Teach your patients the root CBT concept of the cycle of pain, using an illustration connecting pain, distress, and disability.
- Teach your patients to notice the way they think, the types of automatic thoughts, they tend to have, and how these thoughts can impact everything they do. Once patients are aware of their thoughts they can begin to take steps to change them. You can download a useful restructuring sheet at Painpsych.com/Pain-Resources.
- Set concrete goals with your patients to increase their activity level even in the presence of their pain issues. Collaborating with a physical therapist can be an effective way to map progress within the context of a patient’s limitations.
For more information, see:
http://www.painpsych.com/
Otis, JD. Managing Chronic Pain: A Cognitive-Behavioral Therapy Approach, Therapist Guide. Treatments that Work Series. New York, NY: Oxford University Press; 2007.
Otis, JD. Managing Chronic Pain: A Cognitive-Behavioral Therapy Approach, Patient Workbook. Treatments that Work Series. New York, NY: Oxford University Press; 2007.


Recommended


