
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
Suicidality and SSRI’s: An Update
Just when we thought we could finally dismiss the notion that SSRIs cause suicidal ideation, along came the Brits! On June 10, 2003, the British counterpart of our FDA (in Britain, this is the MHRA--Medicines and Healthcare Products Regulatory Agency) issued a "Dear Colleague" letter announcing that Seroxat (the British version of Paxil) should not be used to treat depression in patients younger than 18, because of an increased risk of suicidal ideation.
Before delving into this data in detail, let's step into TCR's time machine to take a view of the research landscape leading up to this event.
In 1990, two years after the FDA approval of Prozac, a group of psychiatrists at Mclean Hospital described 6 patients who developed "intense, violent preoccupations" with suicide within weeks of starting the new medication. While these preoccupations eventually disappeared after stopping the drug, in one case the suicidality continued for three months. A smattering of similar case reports followed on the heals of this one, and suddenly Scientologists and other psychiatry-bashers had a veritable armamentarium to deploy in front of convention centers during APA meetings.
In response, Eli Lilly-funded researchers published meta-analyses comparing large numbers of patients on Prozac with patients on tricyclics, and found no difference in the rates of treatment- emergent suicidal ideation. In fact, most studies of antidepressants, whether funded by industry or academia, have found that antidepressant treatment leads to less suicidal ideation than placebo, as measured by item 3 on the Hamilton Depression Scale--the item that asks patients to rate their degree of suicidality.
More recently, researchers who are "clean" of industry influence have used the Freedom of Information Act to force the FDA to hand over all clinical trial data in their files for each of the "newer" antidepressants (SSRIs plus Effexor, Serzone, Wellbutrin, and Remeron). They found no statistically differences in rate of completed suicides in active drug (0.59%) versus placebo (0.45%). The rate of suicide in the general population is about 0.02%.
What about children and adolescents? We now have data to suggest that the availability of SSRIs has actually led to a decline in adolescent suicide (Olfson, Arch Gen Psychiatry, 2003, 60:978-82). Psychiatric epidemiologists at Columbia University randomly selected 588 zip code regions in the U.S. and examined the relationship between increase in antidepressant prescriptions and decrease in teen suicide rates. They found that a 1% increase in the rate of antidepressant prescribing was correlated with a decrease of 0.23 suicide per 100,000 adolescents per year. This anti-suicide effect was especially prominent in males, in older teens (15- 19), and in lower income neighborhoods.
So, with all this relatively good news as a back drop, what to make of the British rain on our psychopharmacologic parade?
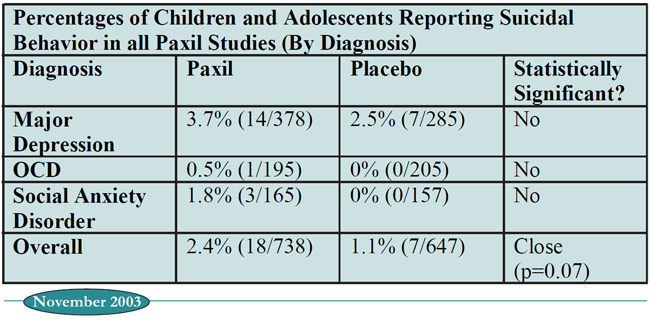
First of all, it is relieving to note that in all of the GlaxoSmithKline (GSK) pediatric trials of Paxil, which involved 1100 patients, there was not a single completed suicide. The table below compiles all existing data on suicidal behavior, published or unpublished, from placebo-controlled trials of Paxil for children and adolescents. As you can see, Paxil seems to cause the most mischief in patients with depression, although even here it does not statistically separate from placebo. It is only when you combine all three diagnostic groups that Paxil begins to look statistically worse.
Table: Percentages of Children and Adolescents Reporting Suicidal Behavior in all Paxil Studies (By Diagnosis)
Ultimately, the FDA will finish their review and come up with a final pronouncement. Until then, you’d do well medico-legally to choose a non-Paxil alternative the next time you prescribe an SSRI to a child.
TCR VERDICT:
SSRIs Don’t Cause Suicide; But Paxil’s been Marked!
General PsychiatryBefore delving into this data in detail, let's step into TCR's time machine to take a view of the research landscape leading up to this event.
In 1990, two years after the FDA approval of Prozac, a group of psychiatrists at Mclean Hospital described 6 patients who developed "intense, violent preoccupations" with suicide within weeks of starting the new medication. While these preoccupations eventually disappeared after stopping the drug, in one case the suicidality continued for three months. A smattering of similar case reports followed on the heals of this one, and suddenly Scientologists and other psychiatry-bashers had a veritable armamentarium to deploy in front of convention centers during APA meetings.
In response, Eli Lilly-funded researchers published meta-analyses comparing large numbers of patients on Prozac with patients on tricyclics, and found no difference in the rates of treatment- emergent suicidal ideation. In fact, most studies of antidepressants, whether funded by industry or academia, have found that antidepressant treatment leads to less suicidal ideation than placebo, as measured by item 3 on the Hamilton Depression Scale--the item that asks patients to rate their degree of suicidality.
More recently, researchers who are "clean" of industry influence have used the Freedom of Information Act to force the FDA to hand over all clinical trial data in their files for each of the "newer" antidepressants (SSRIs plus Effexor, Serzone, Wellbutrin, and Remeron). They found no statistically differences in rate of completed suicides in active drug (0.59%) versus placebo (0.45%). The rate of suicide in the general population is about 0.02%.
What about children and adolescents? We now have data to suggest that the availability of SSRIs has actually led to a decline in adolescent suicide (Olfson, Arch Gen Psychiatry, 2003, 60:978-82). Psychiatric epidemiologists at Columbia University randomly selected 588 zip code regions in the U.S. and examined the relationship between increase in antidepressant prescriptions and decrease in teen suicide rates. They found that a 1% increase in the rate of antidepressant prescribing was correlated with a decrease of 0.23 suicide per 100,000 adolescents per year. This anti-suicide effect was especially prominent in males, in older teens (15- 19), and in lower income neighborhoods.
So, with all this relatively good news as a back drop, what to make of the British rain on our psychopharmacologic parade?
First of all, it is relieving to note that in all of the GlaxoSmithKline (GSK) pediatric trials of Paxil, which involved 1100 patients, there was not a single completed suicide. The table below compiles all existing data on suicidal behavior, published or unpublished, from placebo-controlled trials of Paxil for children and adolescents. As you can see, Paxil seems to cause the most mischief in patients with depression, although even here it does not statistically separate from placebo. It is only when you combine all three diagnostic groups that Paxil begins to look statistically worse.
Table: Percentages of Children and Adolescents Reporting Suicidal Behavior in all Paxil Studies (By Diagnosis)
Ultimately, the FDA will finish their review and come up with a final pronouncement. Until then, you’d do well medico-legally to choose a non-Paxil alternative the next time you prescribe an SSRI to a child.
TCR VERDICT:
SSRIs Don’t Cause Suicide; But Paxil’s been Marked!



Recommended


