
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
CBT for Insomnia
 Chris Aiken, MD.
Chris Aiken, MD. Editor-in-Chief of The Carlat Psychiatry Report. Practicing psychiatrist, Winston-Salem, NC. Dr. Aiken has disclosed that he has no relevant financial or other interests in any commercial companies pertaining to this educational activity.
Each month, Editor-in-Chief Chris Aiken, MD, gives advice on a different practice challenge.
Dear Dr. Aiken: The January 2019 issue mentioned cognitive behavioral therapy for insomnia (CBT-i) as a good alternative to sleep meds. It’s hard to find a therapist trained in CBT-i in my area. Are there any evidence-based self-help options that I can recommend to my patients?
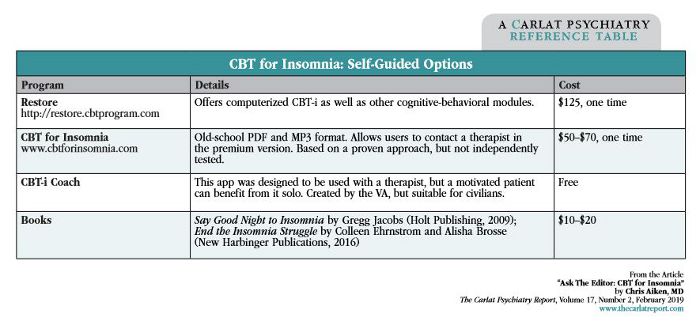
Dr. Aiken: Certified therapists are listed online at www.behavioralsleep.org, but they are few and far between. To bridge this gap, there’s been a lot of research on self-guided CBT-i, and the outcomes suggest it works about as well as the live version (Zachariae R et al, Sleep Med Rev 2016;30:1–10). I’ve collected some of the better-researched programs in the table. My top two options, Sleepio and SHUTi, are on a temporary hiatus and are absent from the table. These programs recently closed their doors to the general public so they can pursue FDA approval as digital therapeutics.
The day may soon come when we’re prescribing CBT-i apps instead of Ambien, and I’ll welcome that. Treatment guidelines already place CBT-i above hypnotics as the gold standard for insomnia. Safety is one reason, but there’s also evidence that CBT-i is more effective over the long term (Beaulieu-Bonneau et al, Sleep 2017;40(3):zsx002). The therapy includes basic sleep hygiene, like avoiding daytime naps, but goes a few steps beyond that. At its core is a structured program of sleep restriction where patients raise their sleep drive by limiting their time in bed. A brief manual is available online at https://tinyurl.com/ycptj345.
General PsychiatryDear Dr. Aiken: The January 2019 issue mentioned cognitive behavioral therapy for insomnia (CBT-i) as a good alternative to sleep meds. It’s hard to find a therapist trained in CBT-i in my area. Are there any evidence-based self-help options that I can recommend to my patients?
Dr. Aiken: Certified therapists are listed online at www.behavioralsleep.org, but they are few and far between. To bridge this gap, there’s been a lot of research on self-guided CBT-i, and the outcomes suggest it works about as well as the live version (Zachariae R et al, Sleep Med Rev 2016;30:1–10). I’ve collected some of the better-researched programs in the table. My top two options, Sleepio and SHUTi, are on a temporary hiatus and are absent from the table. These programs recently closed their doors to the general public so they can pursue FDA approval as digital therapeutics.
The day may soon come when we’re prescribing CBT-i apps instead of Ambien, and I’ll welcome that. Treatment guidelines already place CBT-i above hypnotics as the gold standard for insomnia. Safety is one reason, but there’s also evidence that CBT-i is more effective over the long term (Beaulieu-Bonneau et al, Sleep 2017;40(3):zsx002). The therapy includes basic sleep hygiene, like avoiding daytime naps, but goes a few steps beyond that. At its core is a structured program of sleep restriction where patients raise their sleep drive by limiting their time in bed. A brief manual is available online at https://tinyurl.com/ycptj345.


Recommended


