
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
EXPERT Q&A
Integrating Trauma-Informed Care into Addiction Treatment
 Lydia Bartholow, DNP, PMHNP, CARN-AP
Lydia Bartholow, DNP, PMHNP, CARN-AP
Medical Director, Central City Concern, Portland, OR. Assistant professor, University of California at San Francisco, San Francisco, CA.
Dr. Bartholow, expert for this educational activity, has no financial relationship(s) with ineligible companies to disclose.
CATR: Can you start by introducing yourself?
Dr. Bartholow: I’m a psychiatric nurse practitioner with training in addiction medicine, and I specialize in translating trauma-informed care (TIC) into substance use disorder (SUD) services. I am the medical director at Central City Concern in Portland, Oregon, teach at University of California San Francisco, and am a consultant for organizations looking to make their SUD services more trauma informed, patient centered, and harm reductive.
CATR: What is TIC?
Dr. Bartholow: TIC is a treatment model that starts by recognizing that the bulk of people seeking behavioral health care have experienced adversity in their lives. We assume our patients have experienced trauma and take that into consideration when designing clinical interventions so that the interventions are welcoming, safe, and engaging despite the traumatic experiences. It’s analogous to the model of universal precautions for the prevention of infectious diseases: It’s something we do for all clients that come through our doors. We don’t actually need to know everyone’s trauma history in order to practice in a trauma-informed way.
CATR: How is TIC different from trauma-focused therapy?
Dr. Bartholow: The term trauma-focused therapy refers to a specific group of protocols that treat PTSD, such as cognitive processing therapy or prolonged exposure. In contrast, TIC is a more generalized approach. It’s not about treating a specific diagnosis such as PTSD. A common mistake in organizations trying to build TIC into their systems is that they start screening more intensely for PTSD. Having a clinical practice that is aligned with the principles of TIC doesn’t preclude trauma-based therapy, but instead accommodates all patients, whether or not they have a PTSD diagnosis. Ideally, a trauma-informed system would be set up to easily make internal referrals to trauma-based therapy when needed, but we miss the point of TIC if we are solely focusing on PTSD interventions. It is also important to note that prior adverse experiences don’t necessarily equal PTSD. Many people have difficult experiences yet don’t develop diagnosable PTSD that meets all the DSM criteria—but they can still benefit from a TIC approach. Trauma is associated with increased rates of other disorders, like depression and anxiety, so simply screening for PTSD or increasing access solely to trauma-focused therapy misses these patients.
CATR: Why is it important to provide TIC to patients with addiction? What sort of evidence base is there?
Dr. Bartholow: TIC is a patient-centered approach, and it’s important that we empower patients and include them in treatment planning. Rigorous data, meaning high-powered randomized controlled trials, don’t really exist in this area. Part of the difficulty is that we are not looking at an intervention, but instead we are considering an entire treatment model for how to think through clinical interventions and system designs. Similarly, the outcomes that we are most interested in, like degree of collaboration and feeling safe during treatment, are difficult to quantify. But we do have some observational studies that show that adopting this model can lead to improvement in patient engagement, measures of substance use, patient experience of care, and even work satisfaction among staff who practice TIC (Hales TW et al, Research on Social Work Practice 2019;29(5):529–539). It can re-enliven our work, and this is so important in a post-COVID-19 context regarding burnout among health care workers.
CATR: And there is a large comorbidity between trauma and addiction.
Dr. Bartholow: Yes, that’s true. It makes the trauma-informed model especially relevant for this patient population. There are some really impressive associational data between adverse childhood experiences (ACEs) and the subsequent development of SUDs in adulthood. One study found that patients who had experienced more than six ACEs had a 46-fold increased likelihood of developing an SUD in adulthood (Felitti VJ, Prax Kinderpsychol Kinderpsychiatr 2003;52(8):547–559). That’s an astounding finding, and the strength of the association is at a level we rarely see in public health.
CATR: I’d like to talk a bit about the framework of TIC. It is sometimes presented as adhering to specific guiding principles. Can you explain what those are?
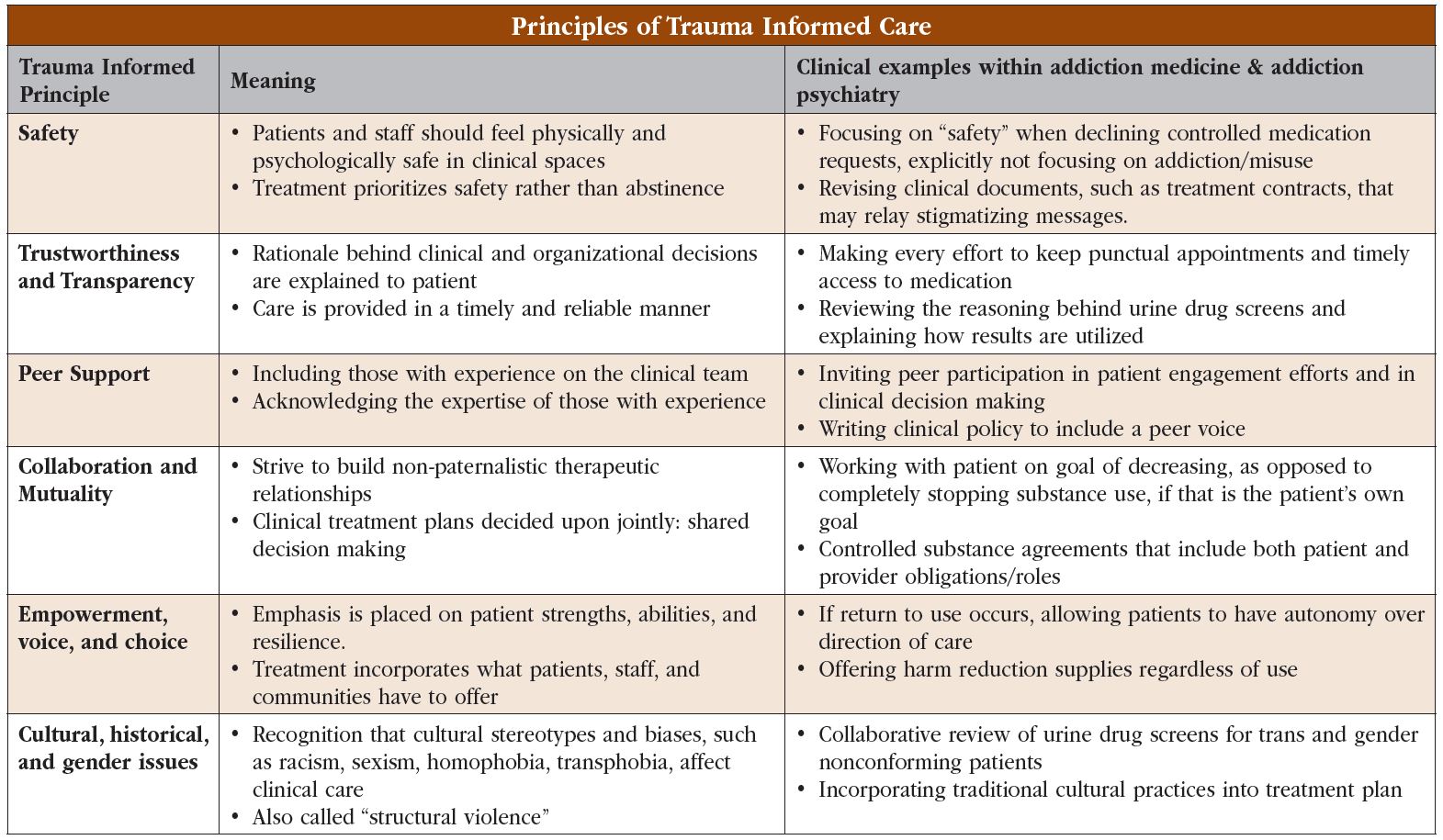
Dr. Bartholow: There are six core principles of TIC: 1) safety; 2) trustworthiness and transparency; 3) peer support; 4) collaboration and mutuality; 5) empowerment, voice, and choice; and 6) cultural, historical, and gender issues. (Editor’s note: See “Principles of Trauma-Informed Care” table below.)
CATR: Could you walk us through the care of a patient, starting with their first visit, to illustrate how TIC can be applied to clinical practice?
Dr. Bartholow: Sure, but I’d like to go even one step back from there, because there are some basic changes to the physical clinic that can help create a trauma-informed environment before a patient even walks in the door. One place for easy changes is clinical signage. One of the core principles I mentioned is collaboration and mutuality. This means we try to avoid highlighting that there’s a power imbalance in the patient-provider relationship. A common signage issue are posters on the wall depicting all the negative impacts of substances on the body, as if patients who use substances don’t already know that they can be harmful. I don’t think patients need shaming reminders every time they walk into the clinic. It’s easy and meaningful to remove that sort of thing and replace it with something warm and welcoming instead.
CATR: Any other changes that can be made to the clinic?
Dr. Bartholow: Furniture arrangement is a big one. Historically, we have prioritized provider safety in our offices, which means being closest to the door. But if we think about the neurobiology of a person who has experienced trauma, we know how close to the surface their fight-or-flight response is. This means ensuring that the patient has easy access to the door. That being said, certain providers may only feel comfortable if they are also close to the door. This translates into giving both patient and provider equal access and should be the default when possible. My personal office setup has the patient closer to the door than me; I have direct access, but the patient is closest. And the very first thing I’ll say to a new patient is, “This is your chair; it’s right next to the door. Would you like the door to be slightly ajar or fully closed?” We should let the patient know that they will have an easy escape if they feel it is necessary and allow them to set their own priority between privacy and the potential discomfort of being closed in a room with a stranger. I believe patients feeling safer can translate into staff safety.
CATR: Once we have a proper clinic set up, then what?
Dr. Bartholow: Then comes the intake process. And in many clinics, that means loads of paperwork. Nobody likes filling out tedious forms, so I try to keep them to a minimum, especially on a patient’s first day. But any time patients are filling out forms, it’s useful to think of that paperwork through the lens of TIC. This is especially true when it comes to controlled substance agreements, which are common in addiction treatment settings. These can be very paternalistic documents, dictating what a patient must do to receive treatment: “You’re not going to share this medicine. You’re not going to sell this medicine. You’re not going to snort this medicine.” But in TIC, we aim to create collaborative language and eliminate language that is shaming or judgmental. I always start with my part of the agreement: “I agree to provide timely refills. I agree to not stigmatize you based on your history of addiction.” And I ask, “Is there anything else that you’d like me to include so that we can be as collaborative as possible?” You can see a sample of my own trauma-informed controlled substance agreement here: www.tinyurl.com/yn78m9we
CATR: It’s emphasizing that the clinician has responsibilities to ensure the success of the treatment as well as the patient.
Dr. Bartholow: Yes, exactly. And those language shifts can be applied to other aspects of clinical encounters. Let’s say I need to talk about what will happen if I’m prescribing methylphenidate to someone with a history of methamphetamine use. I never have a sentence like, “If you resume methamphetamine, your methylphenidate will be stopped immediately.” Instead, I leave space to see what the patient thinks might be the best course of action. I’ll ask, “What do you think I should do if you return to methamphetamine use?” Almost universally, clients suggest the best course of action. I’ve never had anyone say, “Oh, just continue my stimulant.” What they say is, “Well, we should probably stop the methylphenidate, and I want you to encourage me to go back to withdrawal management.” Importantly, we have this conversation at the start of treatment. The clinician and patient document this agreement collaboratively, so if methamphetamine use does occur, we can refer to the prior agreement.
CATR: Isn’t this just good patient-centered care?
Dr. Bartholow: Well, it certainly is good patient-centered care, but in this example, we’re explicitly rooting the conversation in the principles we discussed earlier. TIC is not about always explicitly referencing or calling out trauma; it is about returning to and incorporating TIC principles into these high-stakes clinical moments. In this case we are building our interaction around collaboration and mutuality, and around empowerment, voice, and choice. Again, these are universal precautions, and we use these techniques and approaches for all patients.
CATR: How else can TIC shape clinical encounters?
Dr. Bartholow: Urine drug screens are a good example. Let’s look at a urine drug screen from the perspective of someone who has experienced trauma. They are being told to go into a room, take off part of their clothing, and urinate into a cup, sometimes with a stranger watching. Forcing a patient to do that, especially as a requirement to receive proper medical treatment, can be incredibly activating for someone who has experienced trauma (Scoglio AAJ et al, J Dual Diagn 2020;16(3):347–356).
CATR: I can see how that can be triggering, but how can we get around it?
Dr. Bartholow: First, start by asking yourself if the test is necessary. Many clinicians in the worlds of TIC and harm reduction are moving away from routine urine toxicology. There may be times when testing is useful, but there isn’t compelling evidence that having urine drug screens at every visit improves outcomes—and yet these screens are standard practice in many settings. At one time, urine toxicology was a method for learning whether the “heroin” someone was using contained fentanyl. But now that fentanyl and its analogues have nearly fully infiltrated the opioid supply, screening hardly seems useful for that purpose.
CATR: But drug screens can help monitor treatment response. And there are times it’s clinically necessary, like waiting for a negative opioid screen to start injectable naltrexone.
Dr. Bartholow: Yes, that’s true. And different clinics and providers have their own views and policies on the matter. It’s an area that is actively evolving. But there are ways to make the process consistent with TIC when you do collect a sample. Usually patients are handed a cup and instructed, “Go urinate in this cup.” That’s pretty much it. Depending on the clinical circumstance, there might be someone observing. Instead, we should inform clients about what to expect, hear their concerns, and adjust accordingly whenever possible.
CATR: Can you run us through what that looks like?
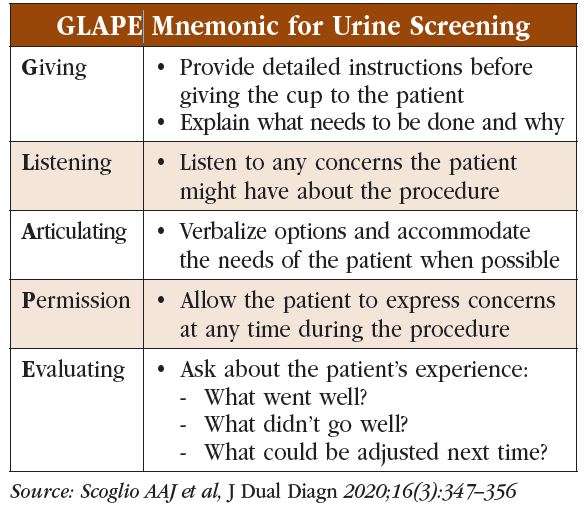
Dr. Bartholow: Sure. There is a mnemonic originally developed for collecting urine drug screens in veterans with co-occurring PTSD (Scoglio et al, 2020). The mnemonic is GLAPE: Giving—give detailed instructions to the patient before you hand them a cup; explain what needs to be done and why. Listening—elicit and listen to any concerns the patient might have about the procedure. Articulating—verbalize options and accommodate the needs of the patient, to the extent possible; for example, if the patient has expressed concerns about being observed, perhaps the sample can be provided unobserved. Permission—allow the patient to express concerns at any time during the procedure. Evaluating—ask about the patient’s experience afterwards. What went well? What didn’t go so well? What could be adjusted for next time? (Editor’s note: See “GLAPE Mnemonic for Urine Screening” table.)
CATR: This is a useful example and seems like it isn’t specific to urine drug screens.
Dr. Bartholow: That’s right; the framework can be applied to all sorts of clinical circumstances.
CATR: We’ve spoken a lot about ensuring patient comfort, but how do we ensure that we aren’t being overly accommodating? We don’t want to fragilize a patient, meaning we actually underestimate their resilience.
Dr. Bartholow: It’s important not to conflate re-traumatization with fragilizing, particularly in SUD care where we know that stigma and poor treatment from medical providers prohibit positive patient experience and engagement. While we don’t want to treat patients like fine china, we do want to avoid shaming and re-traumatizing. When done poorly, any treatment approach, TIC included, can prohibit a belief in recovery and thus stifle it. For example, I have worked with clinics that, in efforts to be trauma informed, require all patients to be screened for ACEs at intake. Unfortunately, this only serves to hyperfocus on trauma history as a way of defining what the patient needs, as opposed to collaborating with the patient—which would be the essence of TIC.
CATR: Where can providers go to learn more about TIC?
Dr. Bartholow: The SAMHSA Treatment Improvement Protocol (TIP) series is excellent, and TIP 57 is a good TIC review. I also really like Trauma Informed Oregon, which is an organization that has done great work around operationalizing TIC into clinical practice. For example, they have straightforward tips on improving urine drug screens to be more trauma informed. Finally, Thomas Jefferson University has videos on their website about engaging people who use substances. They never mention TIC by name, yet what they’re outlining is TIC. They have examples of how to discuss urine drug screen results and perform blood draws on people with a history of IV drug use. (Editor’s note: See “Trauma-Informed Care Resources for Clinicians” table for links to these resources.)
CATR: Thank you for your time, Dr. Bartholow.


Recommended


