
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
CLINICAL UPDATE
Management of Depression and Neurocognitive Impairment in Patients With HIV

Human immunodeficiency virus (HIV) is a retrovirus that causes not only progressive immunologic disease but also neurologic disease. With the advent of effective highly active antiretroviral therapy (HAART), HIV has become a chronic, treatable illness. However, many patients experience mood and cognitive changes, especially if their HIV is poorly controlled. In this article, I will review approaches for the evaluation and management of depression and neurocognitive impairment in patients with HIV.
Depression in HIV-infected individuals
Individuals with HIV/AIDS have more than double the risk for depression compared to the general population, occurring in roughly 30% of patients (Rezaei S et al, BMJ Support Palliat Care 2019;9(4):404–412). Distress from the HIV diagnosis, loss of loved ones to HIV, stigma associated with the virus, HAART side effects, and direct effects of the virus on the brain can all contribute to this high rate.
Assessment
Some depressive-like symptoms—eg, fatigue and poor concentration—might represent medication side effects and HIV-related complications, like HIV-associated neurocognitive disorders. How can we determine whether a patient’s symptoms are due to an underlying depressive disorder? If a patient’s HIV infection is well controlled and their viral load is undetectable, I treat any depressive symptoms as primary depression. In patients with more advanced infections or poor compliance with treatment, lethargy and cognitive impairment may be secondary to the HIV infection rather than depression. Screening for anhedonia, hopelessness, and suicidality will help in reaching the right diagnosis.
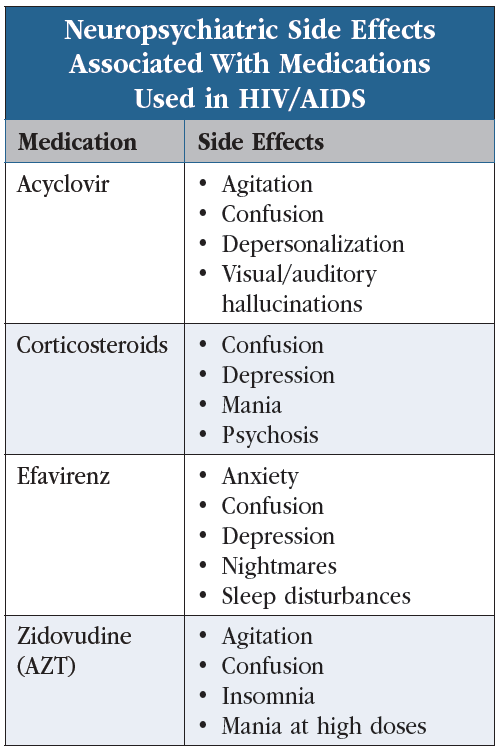
HIV-infected patients are at high risk for suicide, particularly in the days immediately after their HIV diagnosis. Suicide risk correlates most strongly with the development of depression, but several other factors add to this risk, including substance use, personality disorders, and disease progression. The use of certain antiretroviral drugs also increases the risk of depression and suicidality (see “Neuropsychiatric Side Effects Associated With Medications Used in HIV/AIDS” table). It’s important to perform suicide screenings for all patients with HIV, ideally with validated screening instruments such as the Columbia-Suicide Severity Rating Scale (C-SSRS).
 Click to view a full-size PDF
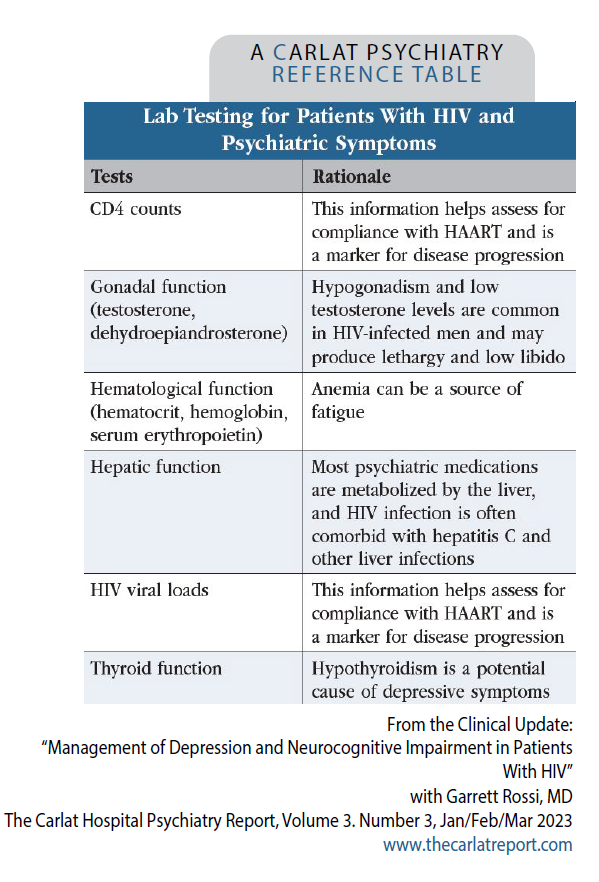
Click to view a full-size PDFMy evaluation focuses on the identification of psychosocial stressors, medication changes, substance use, and the progression of the patient’s HIV infection. I generally obtain hepatic and thyroid function tests, HIV viral loads, CD4 counts, tests of gonadal function (testosterone and dehydroepiandrosterone), and hematological function (hemoglobin, hematocrit, and serum erythropoietin). Why do I obtain these tests? Most psychiatric medications are metabolized by the liver, and HIV infection is often comorbid with hepatitis C and other liver infections, thus a liver function panel can alert us to any hepatic dysfunction. Hypothyroidism is a potential cause of depressive symptoms and should be screened for in this population. CD4 counts and viral loads help assess for compliance with HAART and are a marker for disease progression. Hypogonadism and low testosterone levels are common in HIV-infected men and may produce lethargy and low libido. Testosterone replacement can be considered in severe cases. Anemia can be a source of fatigue, so hemoglobin/hematocrit levels help in the workup of low energy in patients with HIV (see “Lab Testing for Patients With HIV and Psychiatric Symptoms” table).
 Click to view a full-size PDF
Click to view a full-size PDFSome clinicians use screening scales like the Beck Depression Inventory (BDI), but HIV-associated somatic symptoms (eg, fatigue, loss of appetite) might inflate the scales’ scores, potentially causing patients to seem more depressed than they are. The Hospital Anxiety and Depression Scale (HADS) is a validated instrument for detecting depression and anxiety in the hospital or outpatient clinic. HADS scores were found in one study to be unconfounded by the presence of HIV symptomatology and may represent the most reliable and valid screening method for depression and anxiety in HIV patients (Savard J et al, J Pers Assess 1998;71(3):349–367).
Treatment
Psychotherapy and selective serotonin reuptake inhibitors (SSRIs) are first-line therapies for the treatment of depression and anxiety in patients with HIV. Tricyclic antidepressants, which slow gastrointestinal motility and promote weight gain, may be particularly good options for patients with diarrhea and wasting. However, tricyclics are highly anticholinergic and can produce or exacerbate cognitive impairment. Mirtazapine is another option as it stimulates appetite without producing anticholinergic side effects. Bupropion is helpful in cases where fatigue and impaired concentration are primary symptoms, but its dose-dependent seizure risk complicates treatment in patients with neurologic complications from HIV (eg, cerebral toxoplasmosis). I sometimes use psychostimulants, including modafinil, methylphenidate, and dextroamphetamine, as adjunctive treatments for fatigue and apathy when these are refractory to other treatment options.
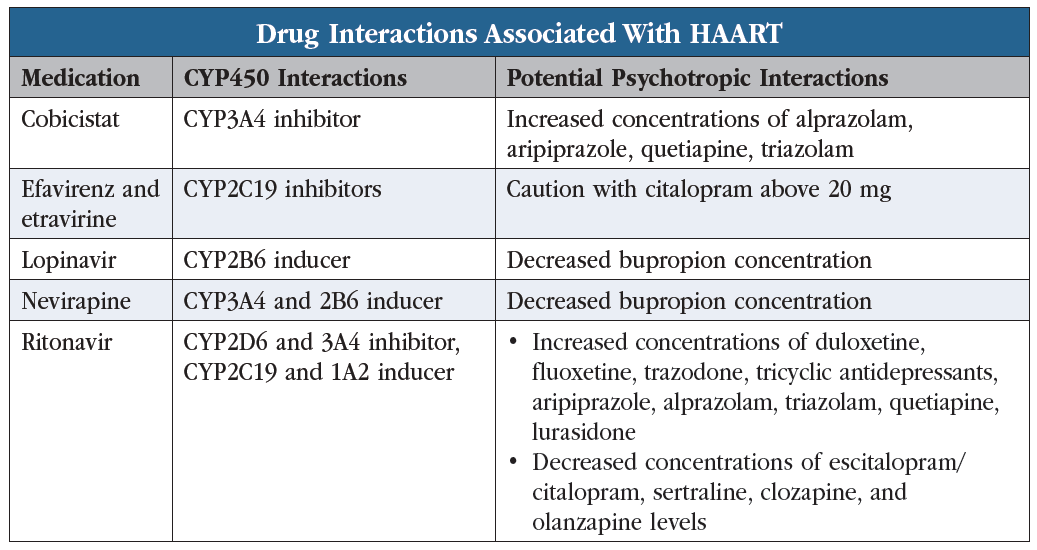
Hypotension is a frequent complication of advanced HIV disease, so I minimize the use of medications that lower blood pressure (eg, prazosin and clonidine). I rarely use ECT for HIV-infected patients due to its risk of cognitive dysfunction, including anterograde and retrograde memory loss. When I prescribe antidepressants to patients on HAART, I try to be mindful of drug interactions (see “Drug Interactions Associated With HAART” table).
 Click to view a full-size PDF
Click to view a full-size PDF
I urge patients to join support groups, as group psychotherapy not only improves depressive symptoms but also enhances social supports, coping skills, and the delivery of HIV education (Nakimuli-Mpungu E et al, Lancet HIV 2015;2(5):e190–e199). A form of cognitive behavioral therapy—CBT for adherence and depression (CBT-AD)—also improves depressive symptoms while enhancing adherence with HAART treatment (Safren SA et al, Health Psychol 2009;28(1):1–10).
HIV and the brain
In case you’ve wondered about the acronym “HAND,” it stands for HIV-associated neurocognitive disorder and encompasses a spectrum of cognitive and functional impairments:
- Asymptomatic neurocognitive impairment (ANI): mild cognitive impairment but no functional impairment
- Mild neurocognitive disorder (MND): mild to moderate cognitive impairment with some functional impairment
- HIV-associated dementia (HAD): severe cognitive impairment with substantial functional disruption
When working with patients with HIV, you will likely encounter some degree of cognitive impairment. The availability of HAART has decreased the incidence of HIV-associated dementia to about 5%, but the prevalence of MND is largely unchanged, affecting about 45% of infected patients (Bhatia NS and Chow FC, Curr Neurol Neurosci Rep 2016;16(7):62). This may be due to patients’ longer life spans and continued viral replication in the central nervous system even when serum levels show undetectable viral loads.
Assessment
In cases of mild or moderate neurocognitive impairment, cognitive screening scales may not be sensitive enough to detect deficits. If I suspect mild or moderate cognitive impairment, I usually obtain formal neuropsychological testing to identify specific areas of dysfunction.
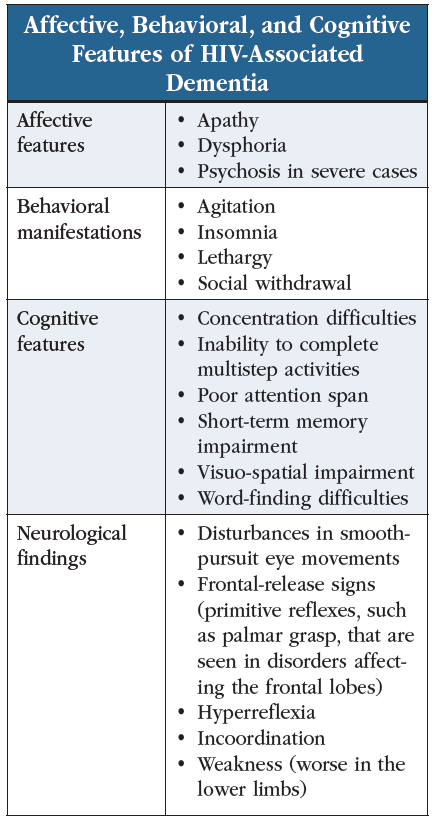
HAD, on the other hand, produces prominent symptoms, including decreased psychomotor speed, poor attention, poor concentration, and impaired memory, learning, and executive function (see “Affective, Behavioral, and Cognitive Features of HIV-Associated Dementia” table). For screening, I recommend the Trail-Making Test as a sensitive and easy-to-use screening tool (www.tinyurl.com/5fx3nw6h). Another instrument, the International HIV Dementia Scale, takes longer to administer but provides a more comprehensive assessment of memory and psychomotor function (www.tinyurl.com/4rmdbbz6).
HAD is a diagnosis of exclusion and thus requires a full workup for other potential causes of the psychomotor slowing (eg, Parkinson’s disease). What typical findings might we encounter in our workup? Neuroimaging often shows cerebral atrophy, enlarged ventricles, and T2-hyperintensities in white matter tracts, and an EEG is likely to show mild background slowing—although I don’t normally obtain an EEG unless I suspect seizures. A cerebrospinal fluid (CSF) analysis will only show nonspecific findings. There’s little reason to obtain a CSF analysis in most cases, but if a patient’s symptoms have progressed rapidly or their CD4 count drops below 100, CSF analysis can help rule out other HIV-related diseases, such as cryptococcal meningitis and toxoplasmosis.
Treatment
The optimal treatment for HAD and HIV-associated neurocognitive disorder is to control viral replication with HAART, as good management of the HIV infection correlates with improved cognitive function (Joska JA et al, J Neurovirol 2010;16(2):101–114). No medications are approved for the treatment of HAD/HAND, but medications for comorbid psychiatric symptoms (eg, agitation) can be helpful.
Potential adverse neuropsychiatric sequelae of HAART
If a patient with HIV demonstrates new-onset cognitive changes or psychiatric symptoms, I look for recent changes to their treatment regimen. Several medications for HIV produce neuropsychiatric disturbances, so I encourage my infectious disease colleagues to take these side effects into account when choosing HAART medications (see “Neuropsychiatric Side Effects Associated With Medications Used in HIV/AIDS”). This is especially important for patients with a history of preexisting psychiatric disorders or with active, poorly controlled psychiatric symptoms. Raltegravir appears to produce a lower risk of neuropsychiatric side effects compared to other options (Kim MJ et al, Infect Chemother 2015;47(4):231–238).
CARLAT VERDICT
Patients with HIV/AIDS are at high risk of depression and suicide, especially in the days following the HIV diagnosis. Many patients with HIV also struggle with cognitive impairment from HAND, and about 5% develop HAD. Psychotherapy and antidepressants help treat patients’ moods, and HAART diminishes the risk of cognitive impairment. Watch for drug interactions and neuropsychiatric side effects from antiretroviral medications.


Recommended


