
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
Clinical Update
What Psychiatrists Need to Know About Intravenous Drug Use and Endocarditis
Infective endocarditis (IE) refers to an infection of the inner lining of the heart, usually of a valve. One of the greatest risk factors for developing IE is intravenous drug use (IVDU), which has become increasingly common since the start of the opioid epidemic in the mid-1990s. Not only can the infection cause heart failure by damaging the valve directly, but microorganisms can spread throughout the body and cause sepsis, stroke, and infarcts in the lungs and spleen. Here, we will review the pathogenesis of IE, signs and symptoms to watch out for, and what to do if you suspect an infection.
Epidemiology
IVDU is on the rise. Currently there are 14.2 million people around the world who inject drugs, with about a million of them in the US (Bradley H et al, J Infect Dis 2020;222(Suppl 5):S218–S229). Over the last 30 years, prevalence of and mortality from IE have both more than doubled—from an estimated 478,000 cases and 28,750 deaths in 1990 to over a million cases and 66,320 deaths in 2019 (Chen H et al, Front Med (Lausanne) 2022;9:774224).
Pathogenesis
In non-IVDU-associated IE, areas with valvular or structural heart disease serve as a place for microbes to attach and grow, forming what is called a vegetation. In patients who don’t use IV drugs, this usually occurs on left-sided valves (aortic and mitral) since pressures there are higher, predisposing those valves to mechanical damage and subsequent bacterial infection.
On the other hand, IVDU-associated IE tends to occur on normal valves exposed to large numbers of microbes entering the systemic circulation through improperly sterilized needles. These microbes travel through the venous circulation and, therefore, usually cause vegetations on right-sided valves (tricuspid and pulmonic). In fact, IVDU accounts for more than 90% of right-sided IE (Moreillon P and Que YA, Lancet 2004;363(9403):139–149).
Signs and symptoms
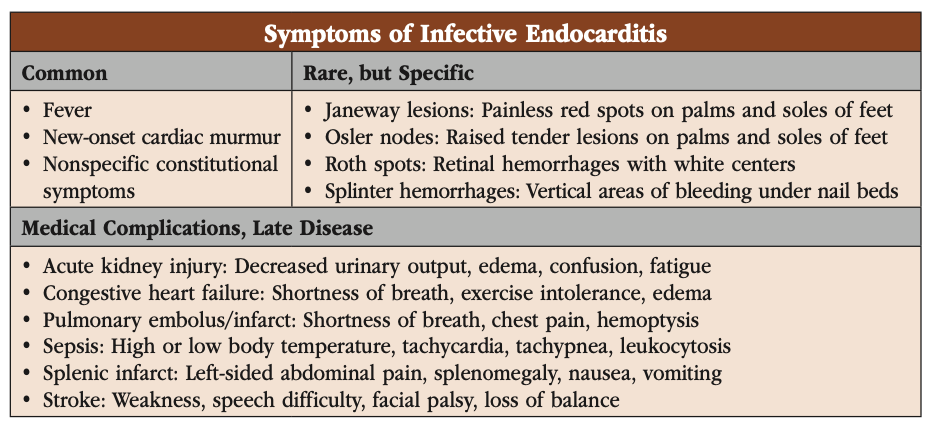
You may recall some of the famous IE clinical findings from your training (or boards exam studying): Janeway lesions, Osler nodes, splinter hemorrhages, and Roth spots (see “Symptoms of Infective Endocarditis” table for an overview of these findings and their symptoms, as well as more common signs and symptoms). Although well known and highly specific, they are actually quite rare.
By far the most common clinical feature of IE is fever, which is present in over 90% of IE patients. It may be constant or it may fluctuate—the pattern is not diagnostically useful. A new cardiac murmur is the second most common clinical finding, occurring in 80% of cases (Murdoch DR et al, Arch Intern Med 2009;169(5):463–473). Other nonspecific constitutional symptoms such as fatigue, night sweats, anorexia, and arthralgias are common as well.
If left untreated, patients may present with medical complications. Valve destruction can lead to congestive heart failure, microorganisms spreading from the vegetation can cause sepsis, and pieces breaking off the vegetation can cause embolic events (see table for more information).
Diagnosis
Most psychiatrists do not perform full physical exams at every visit. Nonetheless, you should have a high index of suspicion when a patient who uses IV drugs appears fatigued or otherwise unwell. At every visit, ask if they have noticed any fevers, unusual fatigue, or unusual skin lesions. If you have the capability to check vitals or listen for a murmur, you should do so, especially if your patients describe any symptoms. An alternative is to refer them to urgently see their primary care provider or go to the nearest emergency room for a workup.
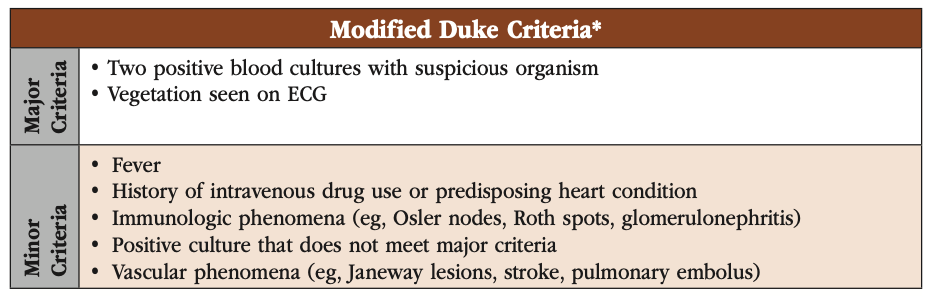
Although you will probably not be ordering the full infectious disease workup yourself, it is useful to know what your patient can expect when they seek treatment. The first step in working up IE is to have an ECG and serial blood cultures. Three or more cultures, which must be separated by at least an hour, are drawn from different sites (Baddour LM et al, Circulation 2015;132(15):1435–1486). From there, a definitive diagnosis can usually be made using the modified Duke criteria, a list of clinical features and laboratory findings broken up into major and minor categories (www.tinyurl.com/thwea6dn; see “Modified Duke Criteria”).
Treatment
The treatment of IE usually begins with long-term antibiotic therapy. The choice of agent will depend on culture results, usually a strain of Streptococcus, Staphylococcus, Enterobacter, or a HACEK organism. Some common antibiotics used are vancomycin, ampicillin, and gentamicin. Cardiothoracic surgeons are needed in complicated cases. Perivalvular abscesses or other severe valvular lesions may require surgical repair or total valve replacement.
IV antibiotic therapy is usually required, sometimes for as long as six weeks. A peripherally inserted central catheter (PICC) line can allow for outpatient antibiotic administration, but it can also be used to inject drugs. Both the inpatient and outpatient teams need to have careful treatment planning discussions with the patient, accounting for substance use disorder treatment engagement, external supports, and stage of recovery, in order to optimize safety and minimize stigma (Morales Y et al, Open Forum Infect Dis 2022;9(190):ofac364).
For patients being treated for IE from IVDU, one of the crucial interventions you can achieve as a psychiatrist is to ensure your patient has access to treatment and practices harm reduction. Discuss treatment options with all patients and make referrals whenever possible. Also, all patients using opioids, IV or otherwise, should receive naloxone. Consider naloxone for patients using stimulants as well, since fentanyl is increasingly being found in non-opioid drugs. And remember that IE is not the only medical complication associated with IVDU. Needle exchange programs have had success in preventing IE as well as other blood-borne pathogens such as HIV and hepatitis C (Bassetti S and Battegay M, Infection 2004;32(3):163–169).
CARLAT VERDICT
IVDU-associated IE is increasing due to the ongoing opioid epidemic. Practiioners who care for patients who use IV drugs should have a high index of suspicion and refer any patients with fever to urgent care or an emergency room for further evaluation. It is essential to make an early diagnosis, since IE carries a high mortality rate if untreated.


Recommended


