
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
Approaches to Autism Intervention

Your patient is a young child who has recently been diagnosed with autism. Her parents are asking about the available treatments, and in particular, they want to know whether they should pursue the 40-hour-per-week program recommended by the local autism society.
As clinicians, we are often faced with questions from families about the “best” program for autism intervention. While children with autism may receive a range of services including speech and language therapy, occupational therapy, and social skills help, some in the community, the anchor to most programs is some form of behavioral health treatment. This article will help you understand the main options for this kind of care and help you advise families on how to proceed.
Three main approaches to autism intervention
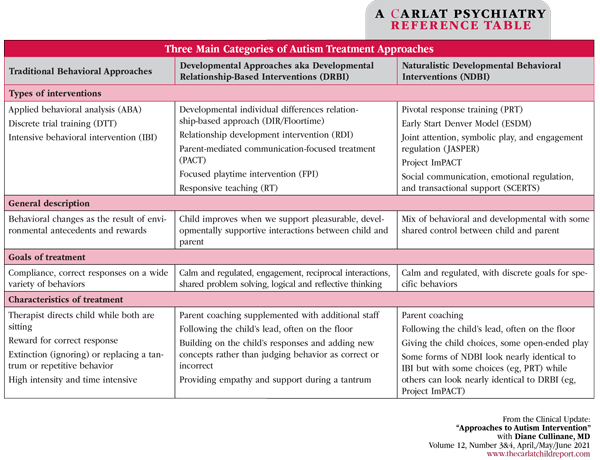
In the past couple of decades, the field of autism intervention has evolved into three main evidence-based approaches. Here’s a brief synopsis of each:
- Applied behavioral analysis (ABA). ABA is the best-known type of intervention. It is based on operant learning theory, meaning that behavior is learned based on what happens before the behavior (antecedent) and what happens after it (reward). Since the groundbreaking 1987 study by Dr. Ole Ivar Lovaas that indicated a positive relationship between individual behavior modification and “normal intellectual and educational functioning,” many additional studies have shown the effectiveness of ABA to help children learn a wide variety of specific behaviors (Lovaas OI, J Consult Clin Psychol 1987;55(1):3–9; Tews L, Developmental Disabilities Bulletin 2007;35:148–168). Some drawbacks of the ABA approach include poor maintenance of skills, poor generalization of learning to new situations, and prompt dependency: reliance on adults to tell the child what to do (Mace FC and Critchfield TS, J Exp Anal Behav 2010;93(3):293–312). See www.bacb.com/about-behavior-analysis for more information.
- Developmental relationship-based intervention (DRBI). In contrast to behavioral intervention, DRBI is a parent-mediated intervention where the primary focus is on training parents and other caregivers to build and use warm, meaningful interactions to help the child function better in communicating, learning, and problem solving. The best-known model is DIRFloortime® or simply Floortime®, which came from the work of Dr. Stanley Greenspan and Dr. Serena Wieder (Greenspan SI, Wieder S. Engaging Autism: Using the Floortime Approach to Help Children Relate, Communicate, and Think. Boston, MA: Da Capo Lifelong Books; 2006). The strategies of developmental interventions are distinct from behavioral intervention approaches in that they are less structured and emphasize free play without direct instruction or contingent rewards. An adult takes a child’s interest and builds on it, while making the activity an emotionally meaningful experience. These fun reciprocal interactions help the child extend their capacities for creating and working with ideas, communicating, and social connection. See www.profectum.org/about/dir and www.icdl.com/dir for more information.
- Naturalistic developmental behavioral intervention (NDBI). In an effort to address some of the drawbacks of traditional ABA, NDBI incorporates more choices for children to gain their buy-in to the treatment. The learning is carried out in natural situations such as play or daily routines and involves parents, and the rewards given are related to the child’s interest. For example, if a child performs the desired behavior, they get the toy they want, rather than a sticker or other reward that other children may prefer. Some goals in NDBIs are chosen based on developmental abilities, such as pointing to share interest (joint attention), eye contact, and having the child imitate an adult, rather than a specific behavior, such as increasing vocabulary. See www.ncbi.nlm.nih.gov/pmc/articles/PMC4513196/pdf/10803_2015_Article_2407.pdf for more information.
In addition, see below for a summary table of these interventions, meant as a start at understanding these different treatments. We recommend that clinicians learn more from the organizations that train and deliver these treatments.
Evidence of efficacy
The most recent edition of The National Clearinghouse on Autism Evidence and Practice supports specific practices that fall within all three of these main branches of autism intervention (Steinbrenner JR, Hume K, Odom SL, et al. Evidence-Based Practices for Children, Youth, and Young Adults With Autism. Chapel Hill, NC: National Clearinghouse on Autism Evidence and Practice; 2020). The American Academy of Pediatrics also endorsed all three interventions in their recent guidelines (Hyman S et al, Pediatrics 2020;145(1):e20193447). While there are thousands of studies on ABA, recent reviews recognize the growing body of research legitimizing DRBI and NDBI and showing that both of these have demonstrable effect sizes for social communication, while these effect sizes have not been shown for ABA (Sandbank M et al, Psychol Bull 2020;146(1):1–29).
Time investment
While mostly focused on younger children, ABA and DRBI approaches are used for children of all ages and abilities and any behavioral challenge. NDBI is more narrowly focused on children 12 and younger. Direct DRBI is usually provided for fewer hours per week than ABA, with parents implementing the model throughout the week, which naturally extends the child’s engagement in the therapeutic process. While DRBI may also employ some additional hours with an interventionist to expand the range of people and experiences the child is exposed to, on balance DRBI requires less time and cost in most cases.
Cost and availability of treatment
The Affordable Care Act mandates that all commercial insurance companies and Medicaid must provide “behavioral health treatment” for autism. Many insurance companies interpret this to mean ABA; however, all evidence-based treatments are included. Though you should direct families to go to their insurance company and ask for the treatment they desire, keep in mind that the choice of intervention approach may be dictated by the available funding source and options available in their community, rather than the best fit for the child and family. Traditional ABA has been easier to obtain with insurance, but developmental options are becoming more available. Good informed consent means the family knows their options. Advocate for their preferred treatment.
Questions from families
As the child’s clinician, your biggest task will most likely be helping the family sort through available treatment options to try and find the best fit for their needs. These common questions and answers should help you respond in a helpful manner.
- Which kind of treatment is best for us? Parents may be baffled by the autism treatment options and the various opinions that they hear. Review the basics of the three types of treatments and help them decide what fits their style and values. For instance, a family that prioritizes learning specific facts and following directions may do better with traditional ABA, and a family that is more free flowing in their interactions may do better with DRBI.
- What’s the main difference between how these different programs work? Behavioral programs are more structured, and the interventionist will work directly with the child to teach them specific skills. They may also teach parents how to use some of these strategies. Developmental programs use natural interactions such as play, focusing on parents’ relationships with their child and on building better communication and learning.
- I am getting different advice from different people—what do I do? Acknowledge that there are many opinions about the “right” treatment for kids with autism. Emphasize the need to figure out what might work best for each family. They can try a treatment out and see how it works. Families often try different styles as their needs change.
- Can we do both ABA and DRBI together? Many children receive some ABA services at school, and developmental services, such as Floortime after school, or other combinations of services. This can be successful if there are clear distinctions about the developmental areas to be addressed. For example, behavioral intervention can focus on specific language or cognitive skills, activities of daily living, or other routines. Floortime could focus on play skills and on interactions with parents and peers. However, confusion can arise if both developmental and behavioral approaches address the same activity, such as feeding, sleep, or behavioral issues. If a child is receiving both types of intervention, work with providers to coordinate their efforts and avoid conflict.
- Where can I get more information? For ABA and NDBI, a good resource is www.bacb.com. For DRBI, good resources include www.icdl.com and www.profectum.org.
CCPR Verdict: Choice of autism intervention is not a one-time decision. It’s an ongoing process of monitoring and evaluation. Any program may be more or less effective depending on the skills of the particular interventionist as well as the match to the family and the developing child. Together, you can guide families in navigating these complex decisions.
Table: Three Main Categories of Autism Treatment Approaches
(Click to view full-size PDF.)


Recommended


