
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
EXPERT Q&A
Treatment-Resistant Depression
 Charles DeBattista, MD
Charles DeBattista, MD
Professor of Psychiatry and Behavioral Sciences, Stanford University, Stanford, CA.
Dr. DeBattista has reported receiving research funding from Relmada, Compass, Janssen, Biolite, Myriad, Neurocentia, Beckley, and Sage, and has served as a consultant for Abvie, Sage, and Corcept. This article was reviewed by Dr. Aiken, Editor-in-Chief, who has concluded that there is no evidence of commercial bias in this educational activity.
TCPR: What is your approach to treatment-resistant depression (TRD)?
Dr. DeBattista: The first step is a good history. Were the trials adequate in dose and duration? How well were they tolerated? What symptoms most bother the patient, and how did they evolve over time?
TCPR: What does the course tell us?
Dr. DeBattista: Most depressions have a gradual onset and offset, but when the episodes cycle frequently or begin and end abruptly, particularly with an onset before the age of 25, it may be a sign of bipolar disorder. Even if they don’t meet full criteria for bipolar disorder, I will look for bipolar spectrum features as these are common in treatment resistance. Patients may have mixed-manic symptoms during the depression, or brief hypomanias that are shorter than the required four-day duration. Psychotic features also raise the risk of treatment resistance, as do comorbidities: substance use, personality disorders, OCD, a history of childhood trauma, and medical disorders (Nemeroff CB et al, Proc Natl Acad Sci U S A 2003;100(24):14293–14296).
TCPR: Which medical disorders do you look for?
Dr. DeBattista: There’s a long list of them, but most are more contributory than causative: cardiovascular and metabolic disease, stroke, obstructive sleep apnea, and inflammatory illnesses like cancer, arthritis, or recent infections including COVID-19. It’s relatively rare that we have a eureka moment in the medical workup, but sometimes we find an endocrine cause like hypothyroidism, Cushing’s or Addison’s disease, or hypogonadism in men.
TCPR: Do you mean low testosterone?
Dr. DeBattista: I’m not talking about the normal decline in testosterone that occurs with age. Testosterone supplementation is controversial there because it may raise the risk of heart attacks and stroke. But when the levels are one or two standard deviations off from the age-adjusted norms, a urology or endocrine consult may be helpful. Also, menopause increases the risk of depression in women, and estrogen can be helpful there (see The Carlat Psychiatry Report October 2020 for estrogen risks and dosing).
TCPR: What do you do when a patient hasn’t recovered after two antidepressant trials?
Dr. DeBattista: You can augment, switch to an antidepressant from a class they have not tried yet, or use an intervention like transcranial magnetic stimulation (TMS), electroconvulsive therapy (ECT), or the ketamines. Some forms of intensive psychotherapy also have evidence, as does aerobic exercise. In terms of medication, augmentation is generally faster and more effective than switching, and the options include second-generation antipsychotics, thyroid, lithium, bupropion, the modafinils, or a dopamine agonist like pramipexole (Nuñez NA et al, J Affect Disord 2022;302:385–400).
TCPR: How do you choose the augmentation agent?
Dr. DeBattista: It depends on the patient’s treatment history and which symptoms are most prominent. Bupropion or modafinil augmentation may be appropriate for someone with low energy and drive. Pramipexole may be helpful for anhedonia. A second-generation antipsychotic may be better for someone who is agitated or has a lot of ruminations or trouble sleeping. For someone who’s struggling with suicidal thoughts, lithium and ketamine or esketamine might be good choices.
TCPR: What would make you lean toward thyroid augmentation?
Dr. DeBattista: There’s some evidence that it works better in women. I tend to consider it for middle-aged women with prominent fatigue, particularly if they have evidence of subclinical hypothyroidism in their labs or elevated antithyroid antibodies (Altshuler LL et al, Am J Psychiatry 2001;158(10):1617–1622).
TCPR: Do you use T3 (liothyronine, Cytomel) or T4 (levothyroxine, Synthroid)?
Dr. DeBattista: Most studies used T3, but either can work. One study compared them head-to-head and found greater benefit with T3, but it was a brief study (three weeks), and T4 may take longer to work because it has a half-life of five to seven days compared to the one-day half-life of T3 (Joffe RT and Singer W, Psychiatry Res 1990;32(3):241–251). I usually start with T3 12.5 mcg/day and titrate to 25–50 mcg/day. The treatment is fairly well tolerated, and side effects like anxiety, tachycardia, and sweating usually improve with dose reduction. With long-term use, there is a concern that osteoporosis can develop, but this has not shown up in the clinical studies and is not a reason to avoid the treatment if the depression is significant. (Editor’s note: See the April 2022 issue of The Carlat Psychiatry Report for more information on thyroid dosing.)
TCPR: Do you dose thyroid by symptoms, labs, or both?
Dr. DeBattista: Both. I check their TSH at baseline and again six to eight weeks later, and I prefer if it doesn’t go to zero. A reasonable target for a TSH level is about 1.0. But at the same time, I’m also looking at whether the patient is getting some relief from their core symptoms.
TCPR: Which antipsychotics work in TRD?
Dr. DeBattista: Some are FDA approved for augmentation: aripiprazole (5–12.5 mg/day), brexpiprazole (2–3 mg), olanzapine (6–12 mg, FDA approved in conjunction with fluoxetine 25–50 mg/day), and quetiapine (150–300 mg). Cariprazine (1.5 mg/day) and risperidone (0.25–2 mg) have good evidence from randomized controlled augmentation trials but are not FDA approved. The challenge with the antipsychotics is that—with the possible exception of quetiapine—there aren’t good long-term studies with any of them in depression (Liebowitz M et al, Depress Anxiety 2010;27(10):964–976).
TCPR: Most of their serious risks rise over the long term, like metabolic problems and tardive dyskinesia. How long do you continue antipsychotic augmentation?
Dr. DeBattista: I think it’s reasonable to try to taper off after six to 12 months of recovery. I’m basing that on the time frame we need to continue an antidepressant after recovery, as this question has not been adequately studied with antipsychotics.
TCPR: Do you find pharmacogenetic testing useful in TRD?
Dr. DeBattista: Several large trials have looked at outcomes with pharmacogenomic-guided treatment, and the results have been mixed, but I think pharmacogenetic testing does have a limited role. For example, the genes that tell us about enzymatic activity in the liver can predict whether some medication levels will go too high, causing side effects, or too low, rendering them ineffective. Many psychiatric medications are metabolized by CYP2C19 and 2D6, like most tricyclics and some SSRIs and SNRIs, so those genes can be informative. A rapid metabolizer at those enzymes may never reach a therapeutic dose, while poor metabolizers may not tolerate the medication or—in the case of tricyclics and citalopram—may develop dangerous arrhythmias with high levels of the drug.
TCPR: Can you tell us more?
Dr. DeBattista: Other genetic tests look at pharmacodynamic markers of response, such as the short allele of the serotonin transporter gene, but it’s not as clear that those genes are useful in predicting response. On the other hand, testing for the B-1502 haplotype in carbamazepine-treated patients is highly recommended as that haplotype is significantly associated with an increased risk of developing Stevens-Johnson syndrome, particularly in individuals of Han Chinese descent.
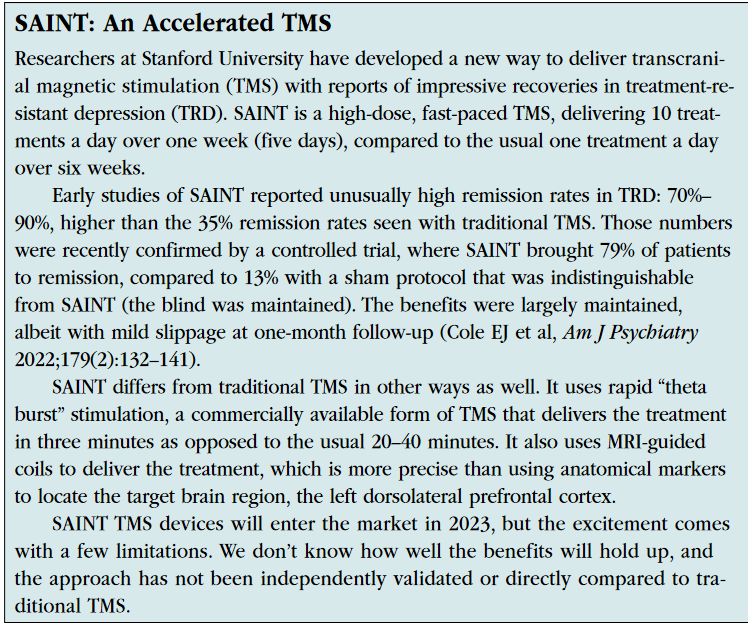
TCPR: Is TMS useful for TRD, or does it only work after one antidepressant failure?
Dr. DeBattista: The original TMS device (NeuroStar) was approved and indicated for depressed patients who had failed at least one but not more than four antidepressants. However, another TMS device (BrainsWay) did gain FDA approval in 2013 for true TRD (two antidepressant failures). Still, it wasn’t until recently that I started to consider TMS for the more severe treatment-resistant cases where historically we’d consider ECT. TMS, like virtually all treatments, works better in less treatment-resistant patients. Our neuromodulation group at Stanford, under the leadership of Nolan Williams, developed an accelerated, five-day protocol that brought remission rates into the 70%–90% range for TRD, and the FDA cleared this “SAINT” protocol last September (see sidebar). Since such a high level of response is almost unheard of in a very resistant population, it will be important to verify these results with independent studies.
TCPR: When should we use the ketamines?
Dr. DeBattista: Their main benefit is that they can quickly reduce suicidality, potentially saving a patient from hospitalization. These drugs—particularly ketamine—have a large effect size in the short term, but they don’t work as well in the long term (Lima TM et al, Eur J Clin Pharmacol 2022;78(3):311–338). Some patients develop habituation or tolerance. That’s what we see clinically, and there are reports of tolerance when ketamine is used for pain management or anesthesia, although in most of that literature the drug was used in a higher dose range.
TCPR: Is there a subset that responds over the long term?
Dr. DeBattista: It’s hard to say as the long-term esketamine trials were not controlled, but some patients swear by it. Typically, it is dosed every one to four weeks when used for maintenance—usually closer to every one to two weeks because the benefits tend to wear off after five to seven days, at least in the ketamine studies.
TCPR: Who is not a good candidate for the ketamines?
Dr. DeBattista: Patients who have a history of psychosis or substance use may not be the best candidates. Ketamine is a PCP derivative, so it can cause psychosis and there are concerns about its abuse potential. Recently I’ve become more careful about patients with a significant trauma history. Ketamine has small studies in PTSD, but we’ve also seen it trigger traumatic reactions: panic, dissociation.
TCPR: Are there any other risks with the ketamines?
Dr. DeBattista: Cystitis and ulcerations in the bladder are common with ketamine abuse, but we haven’t seen that with the lower doses that are used for depression. Acutely, patients can experience nausea as well as increases in heart rate and blood pressure, but these are rarely problematic at the doses used. These drugs are also cumbersome, requiring deliveries from specialty pharmacies and blood pressure monitoring during treatment. Patients have to be driven to and from the appointments and hang around the clinic for about two hours afterwards.
TCPR: You mentioned that we don’t have good support for the long-term use of antipsychotics and ketamines. But in practice it can be hard to stop a treatment after it works.
Dr. DeBattista: We all get complacent about that, but it’s important to have an end point in mind when you start a medication and set those expectations up early. With antipsychotics, you have to reassess for side effects and talk about tapering off if the benefit is no longer worth the risk. With the ketamines, if the patient hasn’t responded within two weeks, we will stop the medication—but if they do respond, the path is less clear. Some of my colleagues continue it indefinitely, but I prefer to tell the patient that we are going to periodically reassess whether it is worth continuing. That depends on their response—are they maintaining a functional recovery or is tolerance developing? It also depends on adverse effects.
TCPR: There are other options with preliminary evidence in TRD: amantadine, celecoxib, minocycline. Where do these fit?
Dr. DeBattista: Among those “off the beaten path” options, the ones I’ve found most helpful have been dopamine agonists like pramipexole, and I would include amantadine in that group although it also affects glutamate transmission. We don’t have much evidence for these, but they may be worth trying in patients who have not responded to multiple trials.
TCPR: A lot of trials focused on patients with mild treatment resistance—patients who failed only two antidepressants or sometimes just failed one. What can we do for those with four or more failures?
Dr. DeBattista: The success rate drops off substantially after several failed medication trials, not just the success rate for medications but also for interventions like ketamine, TMS, and ECT. In the best-case scenario—psychotic depression with no past trials—ECT may have a 90% remission rate in first-episode severe depression, but that may drop to 50%–60% after multiple medication failures. The trials on vagal nerve stimulation (VNS) and deep brain stimulation (DBS) involved more highly resistant depression, but those treatments have ultimately been somewhat disappointing. DBS was not FDA approved for depression because the large registration trials failed. VNS is FDA approved, and though the response rates looked rather low at first (around 30%), they look much better (40%–50%) in the latest studies that include five-year follow-up (Aaronson ST et al, Am J Psychiatry 2017;174(7):640–648).
TCPR: Is VNS a viable option?
Dr. DeBattista: For some. However, many will not respond, surgery is required to implant the device, and those wires are difficult to remove once placed. It also may take a year or two to see the full benefits. We don’t have many takers, actually, but we do have patients in our clinics who have been implanted for a while and have done well.
TCPR: Any tips for working with the psychology of TRD?
Dr. DeBattista: I think one of the biggest challenges for clinicians is falling into the nihilism that many patients with TRD feel. They often become convinced that nothing is going to help, and you can become convinced as well. One of the most important things we offer is hope, and I’ve found there is always something else to try.
TCPR: I still have yet to try d-cycloserine.
Dr. DeBattista: I have actually never tried it either, though it did work in a small controlled trial (Heresco-Levy U et al, Int J Neuropsychopharmacol 2013;16(3):501–506). I have one patient who has tried everything and may be a d-cycloserine candidate.
TCPR: Thank you for your time, Dr. DeBattista.


Recommended


