
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
Clinical Update
The Medical Evaluation of Anorexia
Anorexia nervosa is among the most fatal disorders in psychiatry, with a mortality rate six times higher than that of the general population. For those who require hospitalization, the rate is even higher, with one in 10 dying within five years (Guinhut M et al, Acta Psychiatr Scand 2021;143(2):130–140). Common causes of this mortality include heart failure, arrhythmias, starvation, suicide, and substance use disorders (particularly alcohol and amphetamines). Clinicians can collaborate with medical providers to monitor for these risks, beginning with weight.
How to check weight
Checking height and weight is essential for diagnosis and follow-up. DSM-5 criteria require weight loss to a BMI below “minimally normal,” which is defined as ≤17 kg/m2, although a cutoff of ≤18.5 kg/m2 can be used to identify mild cases. Patients may try to disguise their weight by hiding heavy objects inside bulky or layered clothing, or by loading up on water before the visit.
Whether to share the results of the scale with the patient is a matter of debate. Many programs advocate for blind weighing initially and open weighing as treatment progresses. A patient perspective study found that blind weighing decreased anxiety and weight preoccupation while improving treatment response in the early phases of treatment, but was less important as treatment progressed (Froreich FV et al, J Eat Disord 2020;8:39). However, some believe open weighing serves as a form of exposure therapy that can help extinguish the fear response to weight gain. Federal “open note” regulations will likely shift common practice toward transparency, as the government now requires most physicians to make their notes fully available to patients (see The Carlat Psychiatry Report, June 2021).
Medical assessment
Ask about symptoms that can result from weight loss: fatigue, postural lightheadedness, palpitations, amenorrhea (in female patients), cold intolerance, hair loss, and bone fractures.
In addition to height and weight, the physical examination should include blood pressure, pulse, and temperature. Hypotension, bradycardia, and hypothermia are potential complications of anorexia. Fluid restriction can cause orthostasis, which can be monitored by checking sitting and standing blood pressure.
Common physical exam findings in anorexia include dry skin, yellowing of the skin, lanugo (fine, soft hair similar to that of a newborn), hair loss, irregular heart rhythm, decreased bowel sounds, and peripheral neuropathy.
Although DSM-5 removed amenorrhea from anorexia’s diagnostic criteria, it is common in anorexia and increases the risk of osteopenia and bone fractures. Changes in gonadotrophin-releasing hormone cause hypogonadotropic hypogonadism and low estradiol levels. Estrogen levels are not routinely measured, but a pregnancy test may rule out other causes of amenorrhea.
Osteopenia can develop with or without amenorrhea and occurs in about half of women with anorexia. Testing with dual energy X-ray absorptiometry of the lumbar spine is recommended for those who’ve had anorexia for at least six months.
Laxatives, ipecac, and purging
Around half of patients with anorexia engage in bulimic behaviors, but DSM-5 considers these part of the anorexia diagnosis and does not allow a separate diagnosis of bulimia in these cases. Instead, the diagnosis is “anorexia, binge eating/purging type.” Purging is not limited to vomiting, and patients may not be forthcoming about the full extent of these behaviors, including use of laxatives and diuretics. Compulsive exercise is common in anorexia and does not count toward a purging diagnosis, although exercise does count as a purging behavior in bulimia.
Physical signs of vomiting include parotid gland enlargement, dental caries, and hand abrasions (Russell’s sign). Common complications include esophageal ulcers and electrolyte disturbances, but the medical risks are particularly serious when patients use ipecac to induce a more “complete” vomit. This over-the-counter emetic is used in emergency settings to treat overdoses and accidental poisonings, but ipecac itself is also a toxin. Regular use can be fatal, causing heart failure and rhabdomyolysis (muscle wasting), as in the premature death of singer Karen Carpenter. Ipecac abuse is common in eating disorders and may warrant hospitalization. Suspect it in those with unexplained fatigue and shortness of breath.
Laxative abuse is another form of purging seen in both anorexia and bulimia. Unlike vomiting, which does reduce weight, the only weight loss patients are likely to see with laxatives is from dehydration. Most laxatives work in the large intestine after calories have been absorbed. In addition to dehydration and electrolyte imbalance, laxative abuse increases the risk of colon cancer and urinary tract infections, and it can damage the kidneys, liver, pancreas, and heart. While acute laxative use causes diarrhea, chronic use can cause constipation by damaging the large intestine (Lacey JH and Gibson E, Hum Nutr Appl Nutr 1985;39(1):36–42).
Diuretic abuse is particularly common in athletes with anorexia, who use these dehydrating medications to quickly meet weight requirements. The medical complications of diuretics are mainly derived from electrolyte disturbances, which are discussed below.
Labs
At baseline, check electrolytes, fasting glucose, liver function tests, and complete blood count (CBC). How often to repeat these labs will depend on the severity of illness, particularly the purging behaviors and weight loss. Medical causes of weight loss, like hyperthyroidism, should also be ruled out.
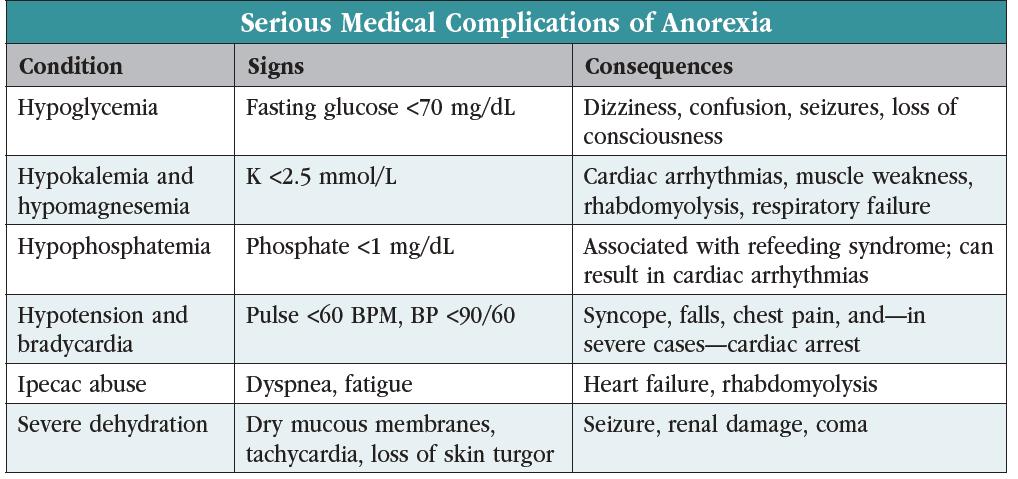
Hypokalemia and hypomagnesemia are common in patients who purge, and these deficiencies can raise the risk of serious cardiac arrhythmias. Purging with diuretics can also lower sodium, leading to flu-like symptoms and—if the sodium is corrected too rapidly—fatal pontine myelinolysis. Abnormal electrolytes should prompt an ECG to check for arrhythmias and QT prolongation. Renal and hepatic function should be checked at the initial assessment but do not require routine follow-up if they are normal. Monitor serum glucose as patients with anorexia are prone to hypoglycemia. CBC with differential can identify potential consequences of neutropenia, leukopenia, anemia, and thrombocytopenia.
Treatment setting
Both psychiatric and medical factors influence the choice of treatment setting. Inpatient or residential treatment should be considered if the patient’s BMI falls below 15 kg/m2. Residential treatment may also be indicated in the presence of psychiatric risk factors such as self-harm or psychosis, inability to eat independently, and low weight despite adequate outpatient measures.
Residential treatment is ideal for the patient who needs more structure and closer management of comorbid psychiatric conditions. Patients in residential care settings should be medically stable, while medical hospitalization is reserved for those with severe symptoms, unstable vital signs, potentially fatal lab abnormalities, and need for constant supervision. Other factors that might call for medical hospitalization include hypokalemia, hypomagnesemia, bradycardia, hypotension, severe dehydration, or ongoing ipecac abuse.
CARLAT VERDICT
The medical assessment in anorexia helps determine an appropriate treatment setting and prevent fatal complications. It includes height, weight, vital signs, a focused physical exam, and labs.



Recommended


