
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
Clinical Update
Capacity Evaluation
You are asked by one of the internists in your hospital to see Ms. Jones, an 86-year-old woman with dementia and severe depression, who is hospitalized with a urinary tract infection. Over the past two days, Ms. Jones has refused to take her antibiotic despite encouragement from her team. Does she have the capacity to refuse antibiotic treatment?
We are often consulted to determine decision-making capacity (DMC) in patients with dementia or other cognitive impairments. This is usually in the setting of a patient who has been admitted for a medical issue and who must make significant decisions about their treatment. How should you go about determining DMC in these cases?
Criteria for DMC
DMC is a fundamental aspect of autonomy. It enables individuals to make their own decisions and exercise control over their lives. Adults are assumed to have DMC, but cognitive disorders like dementia and delirium can reduce this ability to varying degrees and with varying prognoses. Determining DMC is a complex and nuanced process.
When it comes to informed consent, managing finances, living independently, making a will, and driving, patients with dementia can’t be assumed to lack capacity. Instead, DMC must be determined on a case-by-case basis. The process of determining capacity typically involves assessing four key components: communication, understanding, appreciation, and reasoning (Appelbaum PS, N Engl J Med 2007;357(18):1834–1840). See “Components of Capacity Evaluations” table.
A patient’s capacity for a specific decision will depend on their ability to meet all these criteria. However, the level of capacity needed for different decisions can vary. For example, a decision about daily care may require less capacity than a decision about complex medical treatment or major surgery.
Is it capacity or competence?
I often see these terms confused with each other. However, capacity and competence are related but distinct concepts.
Capacity
Capacity refers to a patient’s ability to make a specific decision at a specific time. It’s based on the patient’s cognitive function and the four principles described above. It is not a fixed state and can fluctuate over time, especially in response to medication side effects, delirium, or cognitive decline.
Competence
Competence is a legal determination made by a judge or a court of law, not by clinicians. It’s a finding of a person’s legal ability to make decisions and manage their own affairs. Competence is usually used in the context of guardianship or conservatorship. Criteria to determine competence can vary by country and jurisdiction. In some cases, a person may be deemed competent to make some decisions but not others.
Capacity in people with dementia
Persons with dementia who have preserved awareness of their diagnosis, symptoms, and prognosis are likely to retain capacity to make decisions about their care (Karlawish J, Neurosignals 2008;16(1):91–98). Other patients with dementia may still be able to make decisions related to their daily care, but may not have the capacity to make complex treatment choices, such as creating a living will or making end-of-life decisions.
Here are the steps I take to evaluate capacity in a patient with dementia:
Assess cognitive function
This first step can be done through a variety of tests, such as the Mini-Mental State Exam (MMSE) or the Montreal Cognitive Assessment (MoCA). These tests provide a general assessment of the patient’s cognitive abilities but are not specific for determining DMC. However, in Alzheimer’s disease, an MMSE score below 19 is associated with incapacity, and patients scoring above 23 are very likely to have DMC (Karlawish JHT et al, s2005;64(9):1514–1519). Thus, a patient with an MMSE score of 19–23 may benefit the most from a detailed evaluation of their capacity to make decisions. Keep in mind that cognitive testing may not be as useful among populations without access to higher education, especially racially or economically minoritized populations, as well as among non-native English speakers.
Respect the patient’s autonomy
It is essential to involve the patient in the decision-making process as much as possible. To improve your chances of getting the patient involved, use clear and simple explanations to help them understand the options available and what the consequences of their choices might be. For example, you might say to Ms. Jones: “I see you are not taking the antibiotic. These pills helped you the last time you had an infection. If you stop them now, your infection might continue to make you feel lousy.”
Assess the specific decision using the four principles of capacity
You might say: “Ms. Jones, please tell me why you are in the hospital. Why did you stop taking the antibiotic? What do you think will happen by not taking these pills? What are other treatments for your infection? What are the benefits of the pills? What are the risks of not taking the pills today?”
Involve the patient and their family
The patient’s family members can provide valuable insight into the patient’s baseline decision-making abilities, preferences, and values. Remember to ask the patient for permission before discussing their medical information with others. When your patient is not at their psychiatric baseline, use your professional judgment in determining whether communication is in the best interest of the patient.
For challenging cases, engage a multidisciplinary team
A multidisciplinary team can include a geriatrician, a psychiatrist, a social worker, and/or legal experts such as a bioethics committee to help assess the patient’s capacity and to make recommendations.
Reevaluate regularly
As the patient’s condition changes over time, it’s important to reevaluate their capacity often to ensure that they still have the ability to make decisions. Reevaluation frequency varies based on the underlying cause and expected time course of mental status changes. For example, you might reevaluate daily following an overdose, or every few months in dementia.
Tools for determining capacity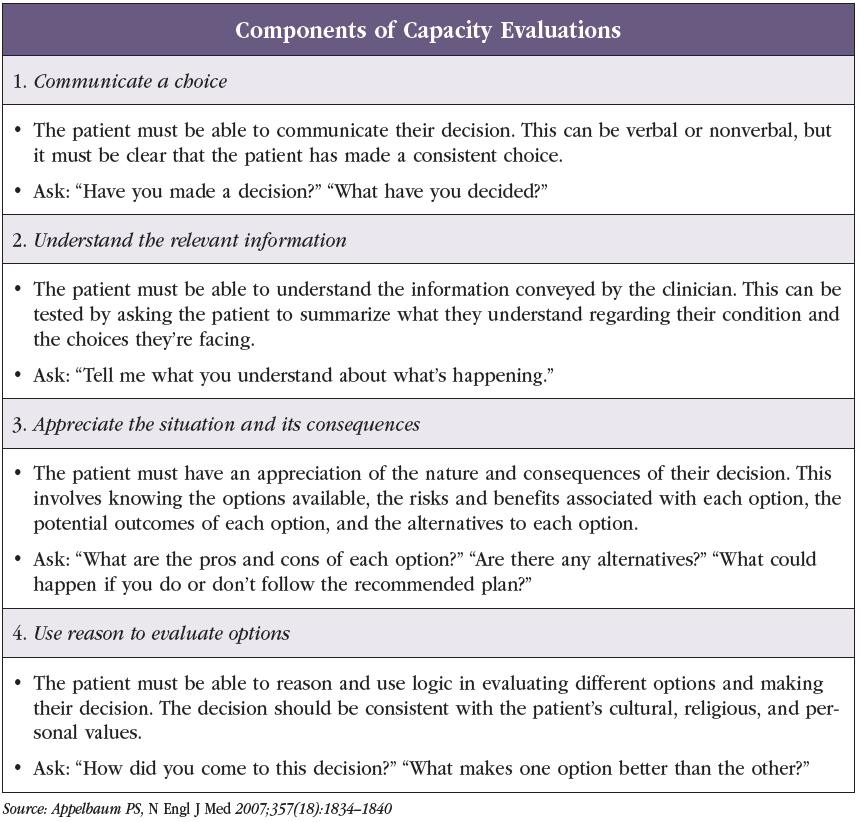
Clinicians can use cognitive screens like the MMSE or MoCA as decision aids, but these screens are not stand-alone diagnostic tools for DMC.
There are several tools that can help assess capacity, but none are universally accepted, and most are lengthy and primarily used in research. One worth looking at is the Aid to Capacity Evaluation (ACE), which aims to help clinicians systematically evaluate capacity when a patient is facing a medical decision. The ACE can be found at the University of Toronto Joint Centre for Bioethics’ webpage (www.tinyurl.com/4bznbpp5) and takes 10–15 minutes to administer.
Ms. Jones scores 15/30 on the MoCA, which is consistent with your concerns about her limited decision-making abilities related to her dementia. You ask her why she does not wish to take her antibiotic, and she expresses concern that her doctors never evaluated her for infection and are giving her the incorrect treatment. You review what happened the last time she stopped her antibiotic (she developed pain when urinating and was medically hospitalized), but Ms. Jones does not think her medications are related to that earlier episode. Despite encouragement from her family, she will not take her antibiotic.
Surrogate decision-makers
If a patient is found to lack DMC after evaluating the four key components of capacity, the next stage is to assign a surrogate decision-maker. A health care proxy (HCP) is a person designated by the patient to make medical decisions on their behalf in the event they cannot make their own decisions. The HCP is invoked when the patient is deemed to lack capacity to make a medical decision. If a patient does not have a designated HCP, family members or loved ones can engage in the legal process of obtaining guardianship to make medical decisions for the patient, although this is often a time-consuming process. In these situations, it’s critical to ensure that the patient is protected from abuse or exploitation.
Although Ms. Jones can communicate her choice, she demonstrates an inability to appreciate the consequences of not taking her medication, and she is unable to provide a logical rationale for refusing it. You determine she does not have capacity to refuse her antibiotic at this time and ask her HCP whether she is in agreement to continue the patient’s antibiotic.
CARLAT VERDICT
Capacity is a clinical assessment that can be supported by standardized measures. Determining capacity requires a careful and individualized assessment of a patient’s understanding of relevant information, communication of a choice, appreciation of the situation, and reasoning abilities. It’s important to strike a balance between respecting a patient’s autonomy and acting on their behalf.



Recommended


