
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
Benzodiazepines for Anxiety: Where They Fit In

Benzodiazepines (BZDs) are widely used, rarely studied, and much maligned. So where exactly do they fit in today’s medication arsenal for treating anxiety? In this article, I will discuss when BZDs are appropriate and when they are not, and how to choose among the various BZDs.
But before doing so, let’s first address the elephant that always seems to be lurking in the BZD room: their addictive potential.
“I’ve heard that benzodiazepines are highly addictive; are they?” It’s one of the most common concerns patients share with me. While BZDs can be abused, the research shows that the vast majority of those abusing BZDs are also concurrently abusing other substances (Busto UE at al, J Clin Psychopharmacol 1996;16(1):51–57).
A task force assembled by the American Psychiatric Association that looked at BZD abuse concluded that the number of patients actually abusing BZDs is “relatively small”—perhaps less than 1% (Rifkin A et al, Am J Psychiatry 1989;146(10):1331–1332). Even most former substance abusers do not appear to be at greatest risk for abusing BZDs (Posternak MA and Mueller TI, Am J Addict 2001;10(1):48–68).
Opioid use, however, presents a clear exception to this rule: Opioid users often report utilizing BZDs specifically to enhance the opioid “high,” and the co-use of opioids with BZDs has negative consequences for general health, treatment outcome, and overdose lethality (Jones JD et al, Drug Alcohol Depend 2012;125(1-2):8–18). BZDs are therefore contraindicated in current opioid users.
What about the fear that BZDs may trigger relapse of other substance use disorders, such as to alcohol? Most research suggests that just the opposite is true. If anything, BZD use may lead to lower rates of substance relapse (Caplan RD et al, Soc Sci Med 1985;21(8):887–898).
Similarly, while it is true that long-term BZD use can induce physiological dependency and withdrawal symptoms, this is not the same as having a substance use disorder. If it were, then paroxetine, venlafaxine, and lithium, among others, would also have to be considered “addictive” medications. Rather, it just means that BZDs need to be tapered off slowly—as is done with many antidepressants and mood stabilizers. For patients who remain hesitant to even try using BZDs, I suggest a limited supply (eg, 10–25 pills per month). I then reassure them, “You can’t get physically dependent on a medication you don’t take every day.”
How to choose among the BZDs
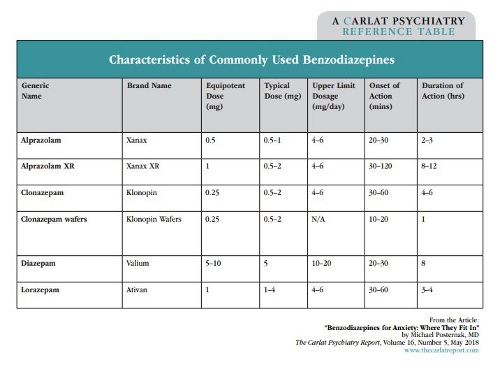
BZDs all share the same mechanism of action: increasing GABA transmission, which has direct anti-anxiety effects, plus sedative effects at higher doses. The main distinction between BZDs is how quickly they work and how long they last. Typically, the faster they kick in, the sooner they wear off; the slower they kick in, the longer they last. The one exception to this rule is diazepam. Because it is lipophilic—meaning it enters fat cells and is slowly released from these cells over time—diazepam works quickly but lasts a long time (this dual feature makes diazepam particularly well suited for treating insomnia).
While there are over a dozen BZDs on the market, you probably will only ever need to use 5 or 6 of the most commonly prescribed ones. These can be ranked from fast-acting to longest-acting in the following order: alprazolam -> lorazepam -> clonazepam -> alprazolam XR.
Diazepam does not fit neatly into this chart because, as stated, it works quickly and lasts a long time. One other BZD that can come in handy is clonazepam wafers. These are taken sublingually and work even faster than alprazolam (alternatively, some clinicians have found that patients can bite traditional BZDs and chew them under their tongue, which allows them to be absorbed more quickly). We will see how these pharmacokinetic differences may affect our choice of BZD depending on the purpose. (For a table of frequently prescribed BZDs and their characteristics, see page 3.)
Prescribing BZDs for anxiety:
The DSM matters!
Anxiety is a fear-driven state of internal distress. It is often useful to distinguish between mental anxiety (worries, ruminations, obsessions) and physical anxiety (chest pain, palpitations, sweating, etc). While patients typically know when they are “anxious,” they don’t necessarily distinguish between various anxiety states. The DSM-5 lists 6 distinct anxiety disorders, and I would argue that the role of BZDs in each specific anxiety disorder is distinct.
As a result, it is not sufficient to simply diagnose your patient as having “anxiety.” Since each disorder may require a different treatment plan, you should always evaluate which anxiety disorders a patient suffers from. In fact, most anxious patients suffer from multiple anxiety disorders. For example, a recent large-scale epidemiological study found that about half of all patients with generalized anxiety disorder have at least 1 other anxiety disorder (Ruscio AM, JAMA Psychiatry 2017;74(5):465–475).
BZDs for each specific anxiety disorder
Panic disorder
Panic attacks are called “panic” for good reason: The sudden onset of overwhelming dread—accompanied by physical symptoms, such as chest pain, palpitations, and shortness of breath—is one of the most crippling experiences patients face. In these situations, patients typically want immediate relief, so the best choice is usually alprazolam (or clonazepam wafers). For many patients, just knowing they have an antidote in their back pocket goes a long way toward staving off future panic attacks. When panic attacks are infrequent, this will typically suffice. But when panic attacks occur more commonly, daily prophylactic medications may be necessary. In these cases, SSRIs may be part of a better long-term solution.
But SSRIs don’t always work, and many patients either do not tolerate them or would prefer to avoid taking daily medications. If so, cognitive behavioral therapy (CBT) should be offered as an alternative. CBT teaches patients how to overcome panic attacks on their own, and therefore—in contrast to medications—can provide an actual cure for panic disorder.
There is one crucial point to keep in mind: CBT only works when patients experience their anxiety. When BZDs help, they actually may prevent the long-term benefits that CBT can offer (Marks IM et al, Br J Psychiatry 1993;162:776–787). Why? Because exposure—both to the feared situation and to the anxiety itself—is the mechanism by which CBT works. If BZDs eliminate patients’ physiological anxiety, then they will not have the opportunity to gain mastery over their anxiety symptoms.
What about patients who want immediate relief from their panic attacks, but also want to engage in CBT so they can get off medications altogether? In these instances, you can offer BZDs now for immediate relief, and in coordination with their CBT therapist, you can plan to wean them off their BZDs. In these instances, the tapering off BZDs becomes the exposure exercise itself: The expectation is that the anxiety may increase during the tapering process. Thus, patients are now choosing to face their anxiety.
Generalized anxiety disorder
Patients with generalized anxiety disorder (GAD) are chronic worriers. Worrying has its advantages, but it can also be extremely taxing. Although SSRIs/SNRIs and buspirone are FDA-approved options for GAD, CBT teaches people how to worry less. Because GAD patients have chronic, daily anxiety, BZDs are not an ideal choice since they would only offer sustained relief when taken daily over an extended period of time. BZDs then are best reserved as a last-resort option for the most severe GAD patients, who have failed on CBT, SSRIs, and buspirone. In these cases, and given its long half-life, alprazolam XR is usually the best option. It can sometimes be dosed once a day, but more often requires BID dosing (typical range 0.5 mg–2 mg QD or BID).
Obsessive-compulsive disorder
Patients with OCD have intrusive, distressing thoughts (obsessions) often associated with compensatory behaviors (compulsions). Despite the high level of anxiety OCD patients can display, BZDs have never been shown to be useful for OCD’s core symptoms, and therefore have no role in treating this disorder.
Social anxiety disorder
Social anxiety disorder (SAD) can range from mild to debilitating, and it can be circumscribed (only manifesting in certain scenarios, such as public speaking) or generalized. Since it potentially limits social functioning and career advancement, more than perhaps any other anxiety disorder, SAD can affect one’s quality of life. Once again, unless the social situation is circumscribed or predictable, CBT and SSRIs will typically be your first-line options. For example, a patient who gets very anxious in meetings may benefit from a BZD 30–60 minutes before that meeting. The same would apply for someone who gets anxious before going on a date (although the patient would need to careful about drinking alcohol) or giving a speech. If physiological symptoms are prominent (particularly palpitations), beta blockers, such as propranolol 20 mg–40 mg, may be a better choice; they are non-sedating and do not impair cognition.
Specific phobias
You may not typically screen for specific phobias. After all, how many patients come in looking for help with their fear of snakes or spiders? But there are two phobias that can be quite debilitating: flying phobias and driving phobias.
Patients presenting for depression (and even anxiety) often will not even mention these phobias unless asked directly. If you do elicit a history of such phobias, you will have the opportunity to make a significant difference in a patient’s quality of life. Maybe a patient hasn’t been able to travel abroad with family, or for years has taken back roads rather than highways to get to work.
CBT can address fear of flying (though SSRIs usually don’t help). But if a patient flies only occasionally, as-needed BZDs are often the perfect solution. They provide consistent relief for most patients that will, at a minimum, allow them to travel wherever they want. For those with more severe anxiety, I use the “sledgehammer” approach: “Take as much medication as you need to reduce your anxiety. As long as you are not driving once you land, the worst that can happen is you will fall asleep during the flight.” Due to its fast-acting nature, alprazolam will usually be the best choice for flying phobias.
In studies, alprazolam has routinely been dosed up to 6 mg/day and, in panic disorder trials, 10 mg/day, so even very high doses are safe. For patients who get anticipatory anxiety, I instruct them to “get ahead of their anxiety,” much as pain patients are instructed to “get ahead of their pain.” This could mean taking alprazolam the night before a flight or on the way to the airport. If the anxiety continues, the patient should keep taking alprazolam every 20–30 minutes.
Since BZDs sedate and affect coordination, driving phobias present a more difficult dilemma.
Nevertheless, I do prescribe BZDs for driving phobias under the following conditions:
What about the risk of an accident? You must discuss this with your patient and document it in your notes, but the reality is that the risk of getting into an accident is probably greater if a patient has severe anxiety than if the patient is taking a BZD that helps alleviate some of that anxiety. For driving phobias, a mid-acting BZD, such as lorazepam or clonazepam, usually works best. Because the risks associated with sedation while driving are inherently greater, it is best to begin with the lowest possible doses and gradually titrate up.
Insomnia
Insomnia is not an anxiety disorder per se, but in many patients who develop acute insomnia, it soon will sound like one. A patient might tell you, “If I don’t get a good night’s sleep tonight, I’m going to be exhausted tomorrow and won’t be able to function at work. I haven’t been able to sleep well in weeks. I don’t know how much longer I can do this!” Here, it is crucial to educate patients about good sleep hygiene habits, with the main principle being to shift the focus away from how many hours of sleep they get, and to focus instead on sleep efficiency (Edinger JD et al, JAMA Psychiatry 2001;285(14):1856–1864). For example, instruct them to get out of bed when they can’t fall asleep after a period of time. Due to the potential for tolerance to develop over time and the risk of dependency, for chronic insomnia it is preferable to avoid BZDs. Trazodone, gabapentin, clonidine, and amitriptyline are good first-line options instead.
But in some cases, such as when insomnia is due to a severe, time-limited stressor, BZDs are the ideal choice. A typical example is the patient who complains of work stress from a looming deadline, leading to late-night racing thoughts and sleeplessness. With such acute distress, there is no need to mess around with other agents: Use a BZD to reduce the nighttime ruminations, and dose it aggressively until adequate sleep is obtained.
Given its quick onset of action and long-acting effects, diazepam is often the ideal choice for insomnia. BZDs generally are pretty “clean” in that they don’t cause much morning grogginess. Should grogginess occur, instruct your patient to take it earlier in the evening, decrease the dosage, or try a shorter-acting BZD. One thing to note, however, is that short-acting BZDs (such as alprazolam and lorazepam) can help patients fall asleep, but they can also induce middle-of-the-night awakenings as the medications begin to wear off. In these cases, switch to a longer-acting BZD.
TCPR Verdict: Benzodiazepines are an invaluable tool for treating anxiety and insomnia. Their abuse and dependency potential are vastly overstated. Use them judiciously, and you can provide tremendous relief for your patients.
General PsychiatryBut before doing so, let’s first address the elephant that always seems to be lurking in the BZD room: their addictive potential.
“I’ve heard that benzodiazepines are highly addictive; are they?” It’s one of the most common concerns patients share with me. While BZDs can be abused, the research shows that the vast majority of those abusing BZDs are also concurrently abusing other substances (Busto UE at al, J Clin Psychopharmacol 1996;16(1):51–57).
A task force assembled by the American Psychiatric Association that looked at BZD abuse concluded that the number of patients actually abusing BZDs is “relatively small”—perhaps less than 1% (Rifkin A et al, Am J Psychiatry 1989;146(10):1331–1332). Even most former substance abusers do not appear to be at greatest risk for abusing BZDs (Posternak MA and Mueller TI, Am J Addict 2001;10(1):48–68).
Opioid use, however, presents a clear exception to this rule: Opioid users often report utilizing BZDs specifically to enhance the opioid “high,” and the co-use of opioids with BZDs has negative consequences for general health, treatment outcome, and overdose lethality (Jones JD et al, Drug Alcohol Depend 2012;125(1-2):8–18). BZDs are therefore contraindicated in current opioid users.
What about the fear that BZDs may trigger relapse of other substance use disorders, such as to alcohol? Most research suggests that just the opposite is true. If anything, BZD use may lead to lower rates of substance relapse (Caplan RD et al, Soc Sci Med 1985;21(8):887–898).
Similarly, while it is true that long-term BZD use can induce physiological dependency and withdrawal symptoms, this is not the same as having a substance use disorder. If it were, then paroxetine, venlafaxine, and lithium, among others, would also have to be considered “addictive” medications. Rather, it just means that BZDs need to be tapered off slowly—as is done with many antidepressants and mood stabilizers. For patients who remain hesitant to even try using BZDs, I suggest a limited supply (eg, 10–25 pills per month). I then reassure them, “You can’t get physically dependent on a medication you don’t take every day.”
How to choose among the BZDs
BZDs all share the same mechanism of action: increasing GABA transmission, which has direct anti-anxiety effects, plus sedative effects at higher doses. The main distinction between BZDs is how quickly they work and how long they last. Typically, the faster they kick in, the sooner they wear off; the slower they kick in, the longer they last. The one exception to this rule is diazepam. Because it is lipophilic—meaning it enters fat cells and is slowly released from these cells over time—diazepam works quickly but lasts a long time (this dual feature makes diazepam particularly well suited for treating insomnia).
While there are over a dozen BZDs on the market, you probably will only ever need to use 5 or 6 of the most commonly prescribed ones. These can be ranked from fast-acting to longest-acting in the following order: alprazolam -> lorazepam -> clonazepam -> alprazolam XR.
Diazepam does not fit neatly into this chart because, as stated, it works quickly and lasts a long time. One other BZD that can come in handy is clonazepam wafers. These are taken sublingually and work even faster than alprazolam (alternatively, some clinicians have found that patients can bite traditional BZDs and chew them under their tongue, which allows them to be absorbed more quickly). We will see how these pharmacokinetic differences may affect our choice of BZD depending on the purpose. (For a table of frequently prescribed BZDs and their characteristics, see page 3.)
Prescribing BZDs for anxiety:
The DSM matters!
Anxiety is a fear-driven state of internal distress. It is often useful to distinguish between mental anxiety (worries, ruminations, obsessions) and physical anxiety (chest pain, palpitations, sweating, etc). While patients typically know when they are “anxious,” they don’t necessarily distinguish between various anxiety states. The DSM-5 lists 6 distinct anxiety disorders, and I would argue that the role of BZDs in each specific anxiety disorder is distinct.
As a result, it is not sufficient to simply diagnose your patient as having “anxiety.” Since each disorder may require a different treatment plan, you should always evaluate which anxiety disorders a patient suffers from. In fact, most anxious patients suffer from multiple anxiety disorders. For example, a recent large-scale epidemiological study found that about half of all patients with generalized anxiety disorder have at least 1 other anxiety disorder (Ruscio AM, JAMA Psychiatry 2017;74(5):465–475).
BZDs for each specific anxiety disorder
Panic disorder
Panic attacks are called “panic” for good reason: The sudden onset of overwhelming dread—accompanied by physical symptoms, such as chest pain, palpitations, and shortness of breath—is one of the most crippling experiences patients face. In these situations, patients typically want immediate relief, so the best choice is usually alprazolam (or clonazepam wafers). For many patients, just knowing they have an antidote in their back pocket goes a long way toward staving off future panic attacks. When panic attacks are infrequent, this will typically suffice. But when panic attacks occur more commonly, daily prophylactic medications may be necessary. In these cases, SSRIs may be part of a better long-term solution.
But SSRIs don’t always work, and many patients either do not tolerate them or would prefer to avoid taking daily medications. If so, cognitive behavioral therapy (CBT) should be offered as an alternative. CBT teaches patients how to overcome panic attacks on their own, and therefore—in contrast to medications—can provide an actual cure for panic disorder.
There is one crucial point to keep in mind: CBT only works when patients experience their anxiety. When BZDs help, they actually may prevent the long-term benefits that CBT can offer (Marks IM et al, Br J Psychiatry 1993;162:776–787). Why? Because exposure—both to the feared situation and to the anxiety itself—is the mechanism by which CBT works. If BZDs eliminate patients’ physiological anxiety, then they will not have the opportunity to gain mastery over their anxiety symptoms.
What about patients who want immediate relief from their panic attacks, but also want to engage in CBT so they can get off medications altogether? In these instances, you can offer BZDs now for immediate relief, and in coordination with their CBT therapist, you can plan to wean them off their BZDs. In these instances, the tapering off BZDs becomes the exposure exercise itself: The expectation is that the anxiety may increase during the tapering process. Thus, patients are now choosing to face their anxiety.
Generalized anxiety disorder
Patients with generalized anxiety disorder (GAD) are chronic worriers. Worrying has its advantages, but it can also be extremely taxing. Although SSRIs/SNRIs and buspirone are FDA-approved options for GAD, CBT teaches people how to worry less. Because GAD patients have chronic, daily anxiety, BZDs are not an ideal choice since they would only offer sustained relief when taken daily over an extended period of time. BZDs then are best reserved as a last-resort option for the most severe GAD patients, who have failed on CBT, SSRIs, and buspirone. In these cases, and given its long half-life, alprazolam XR is usually the best option. It can sometimes be dosed once a day, but more often requires BID dosing (typical range 0.5 mg–2 mg QD or BID).
Obsessive-compulsive disorder
Patients with OCD have intrusive, distressing thoughts (obsessions) often associated with compensatory behaviors (compulsions). Despite the high level of anxiety OCD patients can display, BZDs have never been shown to be useful for OCD’s core symptoms, and therefore have no role in treating this disorder.
Social anxiety disorder
Social anxiety disorder (SAD) can range from mild to debilitating, and it can be circumscribed (only manifesting in certain scenarios, such as public speaking) or generalized. Since it potentially limits social functioning and career advancement, more than perhaps any other anxiety disorder, SAD can affect one’s quality of life. Once again, unless the social situation is circumscribed or predictable, CBT and SSRIs will typically be your first-line options. For example, a patient who gets very anxious in meetings may benefit from a BZD 30–60 minutes before that meeting. The same would apply for someone who gets anxious before going on a date (although the patient would need to careful about drinking alcohol) or giving a speech. If physiological symptoms are prominent (particularly palpitations), beta blockers, such as propranolol 20 mg–40 mg, may be a better choice; they are non-sedating and do not impair cognition.
Specific phobias
You may not typically screen for specific phobias. After all, how many patients come in looking for help with their fear of snakes or spiders? But there are two phobias that can be quite debilitating: flying phobias and driving phobias.
Patients presenting for depression (and even anxiety) often will not even mention these phobias unless asked directly. If you do elicit a history of such phobias, you will have the opportunity to make a significant difference in a patient’s quality of life. Maybe a patient hasn’t been able to travel abroad with family, or for years has taken back roads rather than highways to get to work.
CBT can address fear of flying (though SSRIs usually don’t help). But if a patient flies only occasionally, as-needed BZDs are often the perfect solution. They provide consistent relief for most patients that will, at a minimum, allow them to travel wherever they want. For those with more severe anxiety, I use the “sledgehammer” approach: “Take as much medication as you need to reduce your anxiety. As long as you are not driving once you land, the worst that can happen is you will fall asleep during the flight.” Due to its fast-acting nature, alprazolam will usually be the best choice for flying phobias.
In studies, alprazolam has routinely been dosed up to 6 mg/day and, in panic disorder trials, 10 mg/day, so even very high doses are safe. For patients who get anticipatory anxiety, I instruct them to “get ahead of their anxiety,” much as pain patients are instructed to “get ahead of their pain.” This could mean taking alprazolam the night before a flight or on the way to the airport. If the anxiety continues, the patient should keep taking alprazolam every 20–30 minutes.
Since BZDs sedate and affect coordination, driving phobias present a more difficult dilemma.
Nevertheless, I do prescribe BZDs for driving phobias under the following conditions:
- The patient is engaged in CBT for the driving phobia
- The patient’s anxiety is so impairing that even getting on the road to do CBT driving exercises is a challenge
What about the risk of an accident? You must discuss this with your patient and document it in your notes, but the reality is that the risk of getting into an accident is probably greater if a patient has severe anxiety than if the patient is taking a BZD that helps alleviate some of that anxiety. For driving phobias, a mid-acting BZD, such as lorazepam or clonazepam, usually works best. Because the risks associated with sedation while driving are inherently greater, it is best to begin with the lowest possible doses and gradually titrate up.
Insomnia
Insomnia is not an anxiety disorder per se, but in many patients who develop acute insomnia, it soon will sound like one. A patient might tell you, “If I don’t get a good night’s sleep tonight, I’m going to be exhausted tomorrow and won’t be able to function at work. I haven’t been able to sleep well in weeks. I don’t know how much longer I can do this!” Here, it is crucial to educate patients about good sleep hygiene habits, with the main principle being to shift the focus away from how many hours of sleep they get, and to focus instead on sleep efficiency (Edinger JD et al, JAMA Psychiatry 2001;285(14):1856–1864). For example, instruct them to get out of bed when they can’t fall asleep after a period of time. Due to the potential for tolerance to develop over time and the risk of dependency, for chronic insomnia it is preferable to avoid BZDs. Trazodone, gabapentin, clonidine, and amitriptyline are good first-line options instead.
But in some cases, such as when insomnia is due to a severe, time-limited stressor, BZDs are the ideal choice. A typical example is the patient who complains of work stress from a looming deadline, leading to late-night racing thoughts and sleeplessness. With such acute distress, there is no need to mess around with other agents: Use a BZD to reduce the nighttime ruminations, and dose it aggressively until adequate sleep is obtained.
Given its quick onset of action and long-acting effects, diazepam is often the ideal choice for insomnia. BZDs generally are pretty “clean” in that they don’t cause much morning grogginess. Should grogginess occur, instruct your patient to take it earlier in the evening, decrease the dosage, or try a shorter-acting BZD. One thing to note, however, is that short-acting BZDs (such as alprazolam and lorazepam) can help patients fall asleep, but they can also induce middle-of-the-night awakenings as the medications begin to wear off. In these cases, switch to a longer-acting BZD.
TCPR Verdict: Benzodiazepines are an invaluable tool for treating anxiety and insomnia. Their abuse and dependency potential are vastly overstated. Use them judiciously, and you can provide tremendous relief for your patients.


Recommended


