
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
CLINICAL UPDATE
The 3 Ds of Geriatric Psychiatry: Depression, Delirium, and Dementia
Both common yet elusive, symptoms of depression, dementia, and delirium may overlap in older adults, proving a diagnostic challenge. Even more confounding, these three disorders—the 3 Ds—frequently present simultaneously (Downing LJ et al, Curr Psychiatry Rep 2013;15(6):365). This article will review key features to help distinguish between these disorders and provide tips on their management.
Depression
Older adults may experience “depression without sadness”—this may manifest as anhedonia or somatic symptoms, fatigue, apathy, and general malaise. They are also at higher risk of experiencing psychotic symptoms of depression, with delusions present in up to 45% of older adults admitted to hospitals due to depression (Tampi RR et al, Ther Adv Psychopharmacol 2019;9:2045125319882798). Most commonly, psychotic symptoms manifest as auditory hallucinations (often derogatory comments), paranoia, or nihilistic delusions. When patients experience visual hallucinations, I think instead about delirium, Lewy body dementia, ophthalmological conditions, or brain injury. Patients with an increased vascular burden in the brain and a history of stroke are at a higher risk for developing depression. Depression is also commonly seen as a non-motoric symptom of Parkinson’s disease.
Apathy—a lack of motivation or interest in the absence of a subjectively low mood—may mimic depression and is a common early symptom of dementia.
Assessment
In addition to checking labs to rule out reversible causes of depression (see “Differentiating Among the 3 Ds” table), I screen for sleep apnea using the STOP-BANG sleep apnea questionnaire.
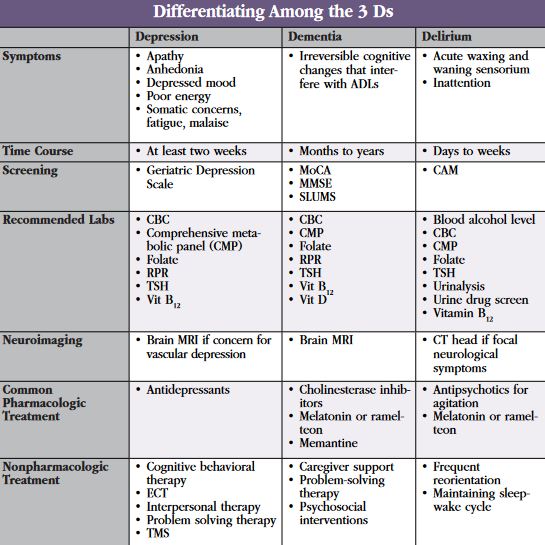
Table: Differentiating Among the 3 Ds
(Click to view full-sized PDF)
The Geriatric Depression Scale (GDS) Short Form is a helpful screener for depression in older adults (www.tinyurl.com/2w944rp4). In patients with no prior history of depressive symptoms, I always ask about subjective cognitive concerns, as late-onset depression can herald a budding neurocognitive disorder. In all patients with depression, I pay attention to suicide risk factors, as older men have the highest risk for completed suicide (Conwell Y et al, Psychiatr Clin North Am 2011;34(2):451–468). (Editor’s note: We will cover suicide risk in older adults in more detail in an upcoming issue of the Carlat Geriatric Psychiatry Report.)
Management
Selective serotonin reuptake inhibitors (SSRIs), serotonin norepinephrine reuptake inhibitors (SNRIs), and mirtazapine are popular first choices. I keep the following saying in mind: “Start low, go slow, but go all the way,” as medications are often underdosed in older adults. As an example, I may start mirtazapine at 7.5 mg at bedtime (or 3.25 mg in frailer patients), increasing in 7.5 mg intervals to a target range of 15–30 mg at bedtime.
Individual psychotherapy interventions, including cognitive behavioral therapy (CBT), problem solving therapy (PST), and interpersonal therapy (IPT), are considered evidence-based practices for late-life depression. Additionally, group therapy can significantly improve symptoms of late-life depression. Consider daily bright light therapy, which may also be effective in non-seasonal late-life depression, or transcranial magnetic stimulation (TMS), although TMS is less effective than electroconvulsive therapy (ECT). For severe or treatment-refractory depression, ECT remains the most efficacious treatment and is well tolerated in the elderly.
Dementia
Dementia is a decline in cognitive function that impacts activities of daily living (ADLs). The most common dementia is Alzheimer’s disease (AD), characterized by the insidious progression of symptoms such as short-term memory loss and word-finding difficulties over the years. When cognition changes over days or weeks, I think of depression or delirium.
Assessment
I screen cognition with one of the following:
- Mini Mental Status Exam (MMSE; www.tinyurl.com/mr2t7xv2)
- Montreal Cognitive Assessment (MoCA; www.tinyurl.com/2p983taz)
- St. Louis University Mental Status Examination (SLUMS; www.tinyurl.com/2p9by8k7)
In addition to the standard dementia labs, think about brain imaging (either head CT or brain MRI), especially if you suspect an atypical course of dementia, see focal neurological signs, or suspect a large vascular burden as a contributor to depression.
Management
I try to optimize nonpharmacological treatments first. These include problem-solving therapies, psychosocial interventions, and caregiver support. Activity scheduling and enhancing daytime structure may improve apathy associated with dementia.
Although cognitive enhancers do not reverse dementia, they may alleviate some of the symptoms. Cholinesterase inhibitors are used for mild, moderate, or severe AD, while memantine is reserved for moderate to severe cases. Melatonin can be helpful for maintaining a normal sleep-wake cycle in patients with dementia.
Delirium
Delirium is an acute confusional state due to a medical illness or its treatment. It develops quickly, usually over the course of hours or days, and fluctuates in severity. Delirium is considered the lupus of psychiatry—it can masquerade as many other psychiatric illnesses. Patients with hypoactive delirium may appear “depressed,” those with hyperactive delirium may appear “manic” or “psychotic,” and those with confusion may appear “intoxicated” or “cognitively impaired.” In patients with delirium, acute changes in environment can lead to rapid behavioral decompensation.
The pathophysiology of delirium involves the dysregulation of multiple neurotransmitter systems, disrupting network connectivity in the brain. Although the community prevalence of delirium is low, it occurs in 10%–30% of hospitalized elderly patients (Gagliardi JP, Virtual Mentor 2008;10(6):383–388).
Assessment
In an older adult with delirium, our priority is to rule out life-threatening causes. I start with a review of a patient’s vital signs and nursing notes to appreciate the time course of the patient’s altered mental status. I review all medications, paying close attention to those known to cause delirium, such as benzodiazepines, anticholinergics, and opioids. I try to rule out infections (UTIs and pneumonias being the most common), electrolyte abnormalities, alcohol or benzodiazepine withdrawal, and other medical illnesses. I also evaluate whether the patient is experiencing pain, hunger, constipation, or changes in sleep patterns. (Editor’s note: For more on assessing and treating delirium in older adults, see article in this issue.)
After thinking through reversible medical causes, I move on to the psychiatric differential. Highest on my differential is dementia—I assume every older adult with delirium has an underlying dementia until proven otherwise. I also consider apathy, depression, and catatonia. To quickly and accurately screen for delirium in older adults, I recommend the 3-D Confusion Assessment Method (CAM) screening tool (www.tinyurl.com/2v295c2w). This screener includes four features that help distinguish delirium from other types of cognitive impairment.
When differentiating between depression, dementia, and delirium, timing is everything (see table). Worsening cognition over days and weeks, in addition to a fluctuating course, is most consistent with delirium. Although dementia progresses over months to years, it can certainly underlie delirium. Delirium (especially hypoactive delirium) can also mimic depression. To disentangle these conditions, testing attention is key—if attention is intact, the patient is not delirious. The fastest way to assess attention is to ask the patient to recite the months of the year (or the days of the week) backwards. If the patient is delirious, remember that no other psychiatric diagnosis can be made in its presence, as delirium holds a place of diagnostic privilege.
Management
Nonpharmacological interventions have the best evidence and can reduce the incidence of delirium by up to 40% (Inouye SK et al, Lancet 2014;383(9920):911–922). I try to keep patients with delirium awake and alert during the day by engaging in activities and conversation, as well as keeping them out of bed if possible. I recommend that windows be kept open to sunlight during the day and that rooms remain dark and relatively undisturbed for sleeping at night. As delirium affects the sleep-wake cycle, wander guards, door alarms, and GPS chips can help ensure patients’ safety in case they wander at night.
I avoid antipsychotics unless physical aggression or psychosis pose a danger to the patient or others. I carefully weigh the benefits of decreasing agitation with the risks of antipsychotics—especially in patients with comorbid dementia, given the FDA’s black box warning of an increased risk of death in individuals with neurocognitive disorders. For physical aggression unresponsive to nonpharmacological strategies, I start with quetiapine 12.5–25 mg or olanzapine 2.5–5 mg either at bedtime or twice daily as needed. I may also consider haloperidol 0.5–1 mg every two to four hours, which has the advantage of availability in PO, IM, and IV formulations. Although antipsychotics can decrease agitation, they have no effect on delirium severity, resolution of other delirium symptoms, or mortality. If an antipsychotic was initiated during an episode of delirium, I try to taper or discontinue the medication once symptoms resolve.
I recommend low-dose melatonin or ramelteon for sleep. Cholinesterase inhibitors do not have a role in the prevention or treatment of delirium, although they can be continued in patients already taking them for dementia. Benzodiazepines, which are deliriogenic, are the preferred treatment for benzodiazepine or alcohol withdrawal.
Finally, I educate family members about the symptoms of delirium and explain how delirium can wax and wane for weeks to months, depending on the severity of the underlying medical condition. To manage expectations, I often mention how patients may or may not return to their cognitive baseline.


Recommended


