
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
Clinical Update
Treating Irritability in Autism: Functional and Medication Approaches
Jane is 10. She watches the children’s program The Backyardigans every morning, mimicking “Hey, they fit together. They do? They do!” When her parents take her electronic device, Jane screams and bangs her head. Her mother tells you, “We can’t live like this.”
Irritability creates substantial distress for autistic individuals and their families. Risperidone and aripiprazole are FDA approved in the US for irritability in autism. While often effective, their side effects include weight gain (even with aripiprazole), neurotoxicity, tardive dyskinesia, and exacerbation of catatonia (Breaux R et al, J Am Acad Child Adolesc Psychiatry 2023;62(3):318–334). This article describes our approach for irritability in autism that minimizes the use of antipsychotic medications.
Set functional goals
Jane’s parents implement a system that links screen time to the behavioral goal “no screaming.” This helps for two days, then the screaming resumes. At your next appointment, Jane says “I get mad and yell.” You suggest a functional goal: “helping Jane feel calm.”
Behavioral goals (used in applied behavioral analysis) aim to change behavior, while functional goals support meaningful interaction. Behavioral goals may bypass underlying factors such as sensory differences, communication problems, and comorbid conditions (eg, anxiety and ADHD). “No screaming” doesn’t address the reasons behind Jane’s screaming. Is she overwhelmed by a busy household or unable to process her parents’ requests? Functional goal setting inspires brainstorming to address underlying factors, which can reduce the use of medications. Other functional goals might include sustaining meaningful interactions, managing sensory differences, or responding adaptively to social problems such as teasing.
Treat co-occurring conditions
Treat co-occurring conditions first as these may drive irritability. Start with non-pharmacologic approaches for conditions such as sleep problems, ADHD, depression, and anxiety. This might include exercise and cognitive behavioral therapy for insomnia (CBTi) modified for autistic patients (eg, using visualization); breaking down tasks for ADHD; and parent-implemented developmental relationship-based intervention (DRBI—see “Related Carlat Resources” table) or CBT for anxiety, depression, or everyday problem solving. Work with colleagues, such as occupational therapists and speech and language pathologists, to address sensory processing, motor planning, and communication challenges, and collaborate with special educators to address challenges related to learning that create frustration and irritability.
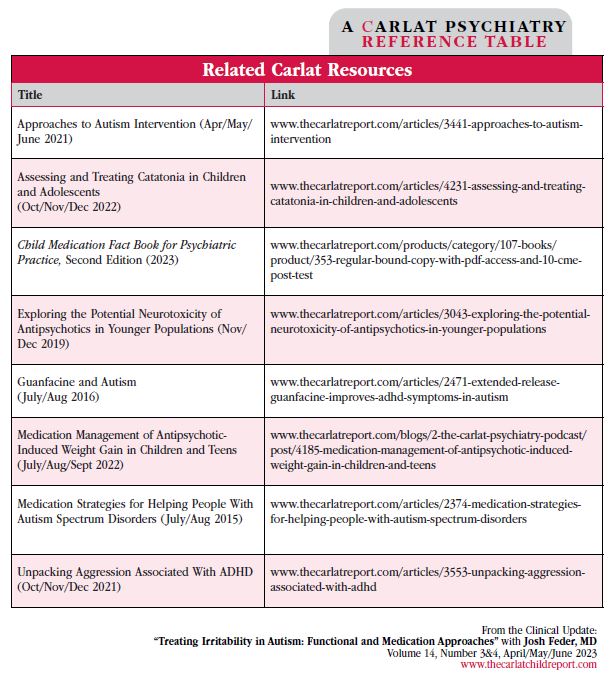
Table: Related Carlat Resources
(click to view full size PDF)
You coach Jane’s parents in DRBI, building on Jane’s interests to help her feel calm. They add brisk morning Backyardigans-styled “treasure hunts,” and Jane is calmer after this meaningful and physical activity. The school reframes Jane’s curriculum around The Backyardigans, making the material more engaging. Jane is better but still anxious.
Off-label medications for irritability
Once you have the non-pharmacologic treatments in place, medications might help, whether for co-occurring conditions or to try to directly address the irritability. Try non-prescription alternatives such as valerian, omega-3 fatty acids, melatonin (daytime), and lavender. They have limited data but might help. If these are ineffective, there is a range of prescription options to consider. Most reports on medication treatments for autism are open label without control groups or effect sizes (see table for more on interpreting research). With that caveat, here are some off-label options ranked within groups from more to less evidence of efficacy.
Neurotransmitter related
Stimulants (dopamine)
Despite negative clinical lore, a recent study suggests stimulants work as well in autistic individuals as anyone else. They have no additional side effects, and at similar dosages for ADHD they may help with irritability and aggression (Lilja MM et al, J Neurodevelop Disord 2022;14(1):17).
SSRIs (serotonin)
SSRIs may help irritability by treating co-occurring depression or anxiety. They generally work better for anxiety than depression for neurotypical kids and teens, but research on SSRIs in autistic children is limited. A recent controlled trial of sertraline for language outcomes in young autistic children ages 24–72 months showed no effect but no significant side effects either (Potter LA et al, Front Psychiatry 2019;10:810). Consider using SSRIs for anxiety, depression, OCD, and repetitive behaviors (after naturalistic approaches). Titrate carefully to avoid behavioral activation.
Memantine (N-methyl-d-aspartate [NMDA] glutamate receptors)
Will decreased glutamate activity reduce irritability? Three controlled trials show memantine is well tolerated and helps receptive language in autistic children (Soorya LV et al, J Child Adolesc Psychopharmacol 2021;31(7):475–484). Maximum dosing is 3 mg daily for kids under 20 kg, 6 mg daily for 20–39 kg, 9 mg daily for 40–59 kg, and up to 15 mg daily for 60 kg and over (Aman MG et al, J Child Adolesc Psychopharmacol 2017;27(5):403–412).
Bumetanide (GABA)
Animal autism models have increased GABAergic activity. What about decreasing GABA tone with bumetanide? In the only controlled human trial, bumetanide showed no effect on irritability or other autism symptoms (Sprengers JJ et al, J Am Acad Child Adolesc Psychiatry 2021;60(7):865–876). Recommendation? Skip it.
Autonomic approaches
Guanfacine
This central alpha-agonist reduces sympathetic tone, fostering calm, with occasional dizziness or paradoxical irritability. A 2015 study demonstrated that, for ADHD symptoms, about half of autistic children improved with few side effects (Scahill L et al, Am J Psychiatry 2015;172(2):1197–1206). Start at 1 mg daily and titrate to 4 mg daily, or 2 mg for kids less than 90 lbs.
Propranolol
This beta-blocker reduces racing heart rate to lower anxiety but may also lower exercise tolerance or exacerbate asthma. A 2016 controlled pilot study using a single dose of propranolol showed improved conversational reciprocity in autistic kids, and if effective would presumably help problem solving and therefore irritability (Zamzow RM et al, Psychopharmacology (Berl) 2016;233(7):1171–1178). Dose at
5–10 mg daily, increasing by 5 mg weekly, usually to a maximum of 20 mg daily.
Hormonal
Balovaptan
This medication blocks central vasopressin activity. A preliminary double-blind placebo-controlled study in autistic children ages 6–12 years showed improved social function and reduced anxiety (Parker KJ et al, Sci Transl Med 2019;11(491):eaau7356). We want more research before recommending it.
Oxytocin
This “bonding hormone” is a non-starter since multiple adult autism trials have failed (Sikich L et al, N Engl J Med 2021;385(16):1462–1473).
Opioid system
Low-dose naltrexone (LDN). Small older studies show that LDN may help irritability in autism. If you try it, titrate to 3–5 mg daily and watch LFTs (Salazar de Pablo G et al, J Am Acad Child Adolesc Psychiatry 2022;62(2):151–168).
Trials of guanfacine and low-dose fluoxetine have no impact on Jane’s irritability, so you try low-dose (0.5 mg) naltrexone. The medication requires compounding, insurance does not cover it, and the cost is beyond what the family can afford.
Social determinants
Culture and other social determinants can impact off-label prescribing in autism: Some medications are too expensive, and approval of prior authorizations may be difficult without definitive research. Families may mistrust the medical system and view off-label “experiments” in a context of historical injustices (www.tinyurl.com/4mj8zyvr). Listen and offer neutral information and perhaps these concerns will abate. Offer options based on your clinical judgment and existing research and let families choose based on their culture, values, and circumstances.
You ask the pharmacy to discount the naltrexone price and they agree. Jane is calmer and engaging better with others. Six months later, her parents report that she is learning and building friendships.
Escalating to antipsychotics
If your patient remains significantly irritable, consider moving to antiepileptic drugs (eg, gabapentin, oxcarbazepine, valproate, or topiramate). If irritability is persistent or severe, consider antipsychotics that are less metabolically problematic, such as ziprasidone or lurasidone. Note that if the patient’s symptoms meet criteria for bipolar depression, it may be easier to get insurance funding for lurasidone if they are age 10 years or older. Reserve risperidone and aripiprazole for severe or intractable situations, and think about using metformin early to help forestall metabolic effects. Track metabolic parameters and abnormal movements. Finally, think about discontinuing the medication when possible (see table for more information).
There are many potential underlying reasons for irritability in autism, and your approach should try to address those issues and avoid escalation to antipsychotics if possible. Start by trading behavioral goals for meaningful functional goals and implementing non-pharmacologic supports. Consider milder offlabel medications and ones with low metabolic impact before turning to the FDA-approved antipsychotics. For a diagrammatic algorithm, see the new edition of our Child Medication Fact Book (Feder J et al. Child Medication Fact Book for Psychiatric Practice. 2nd ed. Newburyport, MA: Carlat Publishing; 2023).
CARLAT VERDICT
There are many potential underlying reasons for irritability in autism, and your approach should try to address those issues and avoid escalation to antipsychotics if possible. Start by trading behavioral goals for meaningful functional goals and implementing non-pharmacologic supports. Consider milder offlabel medications and ones with low metabolic impact before turning to the FDA-approved antipsychotics. For a diagrammatic algorithm, see the new edition of our Child Medication Fact Book (Feder J et al. Child Medication Fact Book for Psychiatric Practice. 2nd ed. Newburyport, MA: Carlat Publishing; 2023).



Recommended


