
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
Clinical Update
Dextromethorphan Misuse
Getting your Trinity Audio player ready...
Michael is a 19-year-old college student brought to the ED after friends found him confused, agitated, and hallucinating. His heart rate and blood pressure are significantly elevated, and his pupils are dilated. His routine urine drug screen is negative, and the diagnosis is a mystery until his roommate mentions that he found several empty boxes of cough medication in their room.
Dextromethorphan (DXM) is a widely available antitussive found in more than 125 over-the-counter (OTC) cough and cold remedies. At standard doses, up to 120 mg/day, it’s safe and typically causes few side effects. But at high doses, DXM can act as a dissociative hallucinogen with psychoactive effects similar to other dissociatives like ketamine and PCP. Although DXM is largely unregulated, misuse can lead to severe toxicity, psychiatric complications, and even death.
Recreational use, sometimes called “robotripping,” “skittling,” or using “Triple C’s,” is especially common among adolescents and young adults. DXM misuse can be easy to miss: It’s not detected by standard urine drug screens, and purchases aren’t tracked by prescription drug monitoring programs. Many patients don’t volunteer information about their use, and clinicians may overlook it.
Epidemiology
DXM misuse has been reported globally but is most prevalent in the US, Canada, Japan, and Europe, with adolescents at highest risk. In the US, teens and young adults aged 12–20 are three times more likely than adults to present to the ED for DXM-related problems (Brown GR et al, JAAPA 2018;31(8):1–5). In a systematic review of published cases, about one-third of people who misused DXM also had another substance use disorder (SUD). In addition, about a quarter had a mood, psychotic, or anxiety disorder, so patients found to be misusing DXM should be assessed for psychiatric comorbidities (Schifano F et al, Front Psych 2021;12:357397).
Mechanism of action and toxicity
DXM is structurally related to opioids but does not activate mu-opioid receptors at normal doses. Its psychoactive effects come from dextrorphan, a metabolite formed via CYP2D6 metabolism that acts as a noncompetitive N-methyl-D-aspartate (NMDA) receptor antagonist. Like other NMDA receptor antagonists, such as ketamine, moderately high doses of DXM can produce pleasant stimulant and euphoric effects. But as the DXM dose increases, users can experience agitation, powerful dissociation, hallucinations, and dangerous autonomic activation.
Genetic differences can affect the rate of drug metabolism and downstream effects. Ultra-rapid metabolizers may experience intense short-lived effects, while poor metabolizers may have prolonged toxicity at low doses. CYP2D6 inhibitors like fluoxetine, paroxetine, and bupropion can increase DXM levels and duration of action as well (Journey JD et al. Dextromethorphan Toxicity. Treasure Island, FL: StatPearls; 2023).
DXM also directly inhibits serotonin reuptake at high doses, making serotonin syndrome a concern, especially when combined with selective serotonin reuptake inhibitors or other serotonergic agents. Finally, DXM inhibits peripheral reuptake of adrenergic neurotransmitters, resulting in tachycardia, elevated blood pressure, and diaphoresis.
- Toxicity is dose dependent and can be conceptualized as four “plateaus”:
- First plateau (100–200 mg): Restlessness, mild stimulant effects, sense of intoxication
- Second plateau (200–400 mg): Euphoria, perceptual changes, slurred speech
- Third plateau (400–600 mg): Dissociation, ataxia, hallucinations, time distortion
- Fourth plateau (>600 mg): Delirium, psychosis, seizures, coma
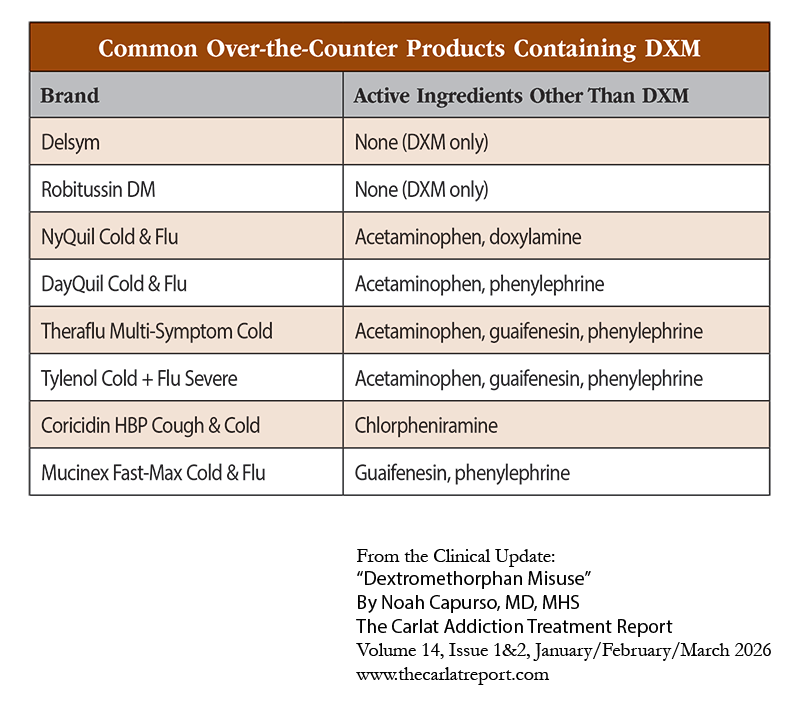
Moreover, many DXM products contain other medications, which may compound toxicity. Common additives include acetaminophen (hepatotoxicity), the anticholinergics chlorpheniramine and doxylamine (anticholinergic delirium), and pseudoephedrine (tachycardia or hypertension). See “Common Over-The-Counter Products Containing DXM” table on page 9 for an overview of the additional medications included in some formulations.
Recognition and diagnosis
Suspect DXM misuse when you see a young, otherwise healthy patient with acute-onset hallucinations, dissociation, or psychosis, especially in the presence of elevated vital signs and a negative urine drug screen. Additionally, look for signs of anticholinergic toxicity, such as mydriasis, tachycardia, or dry mouth. Obtain collateral from the patient’s family or friends if possible.
Don’t hesitate to ask about DXM directly, but keep in mind that patients may not be immediately forthcoming. Just as when asking about use of any substances, maintain an open curiosity and avoid judgmental language. For example:
- “People sometimes use cough syrup that you buy at the store in ways other than directed. Is that something you’ve tried yourself?”
- “Along with prescription and recreational drug use, I always ask about use of OTC medications like cough medicine because they can affect your health too. Have you ever taken OTC medications in ways that are not recommended?”
Clinical management
For mild symptoms, close observation, supportive care, and reassurance are usually sufficient. Moderate to severe cases may require a more comprehensive treatment plan, especially when co-ingestants or psychiatric symptoms are present. If the ingestion is within 1–2 hours, activated charcoal may be helpful in large doses, particularly for formulations that include acetaminophen. Otherwise, supportive care is first line. Monitor vitals, hydration, and hepatic and renal function. A quiet environment can help manage anxiety and mild agitation.
For psychosis or severe agitation, start with benzodiazepines (BZDs), such as lorazepam, and proceed to second-generation antipsychotics such as olanzapine if symptoms persist. Exercise caution if using first-generation antipsychotics and parenteral formulations given the risk of worsening hyperthermia and anticholinergic toxicity (Zaremba M et al, Biomedicines 2023;11(1):123).
Seizures warrant immediate parenteral BZDs and a neurology consult as severe cases can progress to status epilepticus (Okamoto A et al, Am J Case Rep 2025;13(26):e946447). Respiratory suppression is rare but can be seen in large ingestions. For these patients, consider administering naloxone. While it isn’t standard practice, naloxone has a good safety profile and there are some case reports of its efficacy (Kumar D et al, Cureus 2023;15(2):e34501).
Finally, in addition to the mental status changes, watch out for signs of serotonin syndrome, including hyperthermia, hyperreflexia, rigidity, and clonus. Treat suspected serotonin syndrome promptly (see CHPR January/February/March 2021 for more on serotonin syndrome diagnosis and management).
Dependence risk and long-term effects
DXM doesn’t create the same level of physical dependence as opioids or alcohol, which can cause withdrawal symptoms severe enough to require hospitalization. Nonetheless, people who chronically use DXM can develop tolerance and experience withdrawal symptoms such as dysphoria, craving, insomnia, and gastrointestinal upset. Some patients, particularly those with chronic use or who also take serotonergic agents, may experience psychosis that lasts well beyond the period of acute intoxication. Most recover in a few days, but some may require psychiatric hospitalization for weeks or even months (Schifano et al, 2021; Zaremba et al, 2023).
Those who use DXM chronically can meet criteria for an SUD as well. Very little research has been done into treatment for those who misuse DXM, but some early reports suggest potential roles for naltrexone, topiramate, and gabapentin in withdrawal and maintenance treatment (Schifano et al, 2021; Ledwos N et al, Am J Drug Alcohol Abuse 2023;49(2):266–267).
Michael is monitored closely in the ED. He responds well to supportive care and several doses of lorazepam to treat his anxiety. His hallucinations are self-limited and resolve after 24 hours. He is discharged back to his dorm and referred to an outpatient psychiatrist, who begins treating him for depression and anxiety.
Carlat Verdict
DXM is a common OTC medication that can cause severe psychiatric and medical complications when taken in high doses. While evidence for treatment is limited, supportive care, BZDs, and select antipsychotics can be effective, as well as naloxone in severe cases involving respiratory suppression. Remember to ask patients about OTC medication use and maintain a high index of suspicion, especially in young patients with unexplained psychosis or agitation.



Recommended


