
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
Traumatic Brain Injury: Definition, Classification, and Management
We hear a lot about traumatic brain injury (TBI) nowadays: among NFL players (as in the movie ‘Concussion’), and as a signature diagnosis among recent combat veterans. What doesn’t get as much press coverage is the impact of TBI on those suffering from addiction. Having an alcohol or other substance use disorder greatly increases the risk of TBI. But what is TBI? How do I diagnose it? How does it manifest? How do I manage it?
Defining TBI
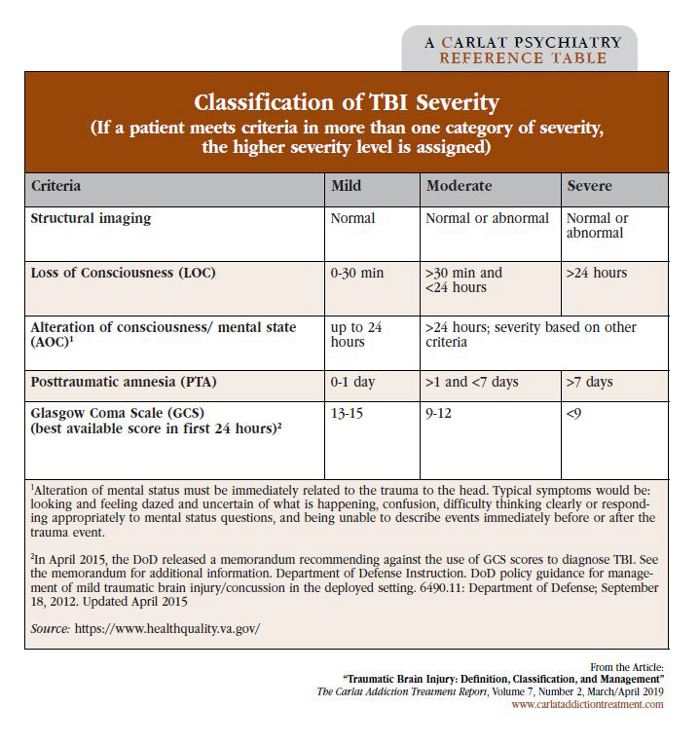
Although there is no universally accepted definition for TBI, recently updated guidelines from the Department of Veterans Affairs (VA/DoD Clinical Practice Guideline for the Management of Concussion-mild Traumatic Brain Injury, 2016; https://tinyurl.com/y8e6owdx) state that a TBI is an injury to the brain caused by an external force accompanied by one of several clinical signs following the event). These signs can be an intracranial lesion, loss of consciousness, amnesia, confusion, slowed thinking, muscle weakness, sensory loss, or another neurological deficit. The severity of a TBI (mild, moderate, or severe) is determined by the symptoms immediately following the injury (see the VA TBI severity table below). If the patient meets different ratings for the different criteria, go with the more severe rating. The lay term “concussion” equates to a mild TBI. In addition to the neurological symptoms, patients may experience cognitive problems affecting their attention, memory, processing speed, and executive function. Mental health effects include irritability, impulsivity, depression, and anxiety. However, these symptoms can be an effect of the TBI or part of a comorbid, major depressive disorder, posttraumatic stress disorder (PTSD), or substance use disorder.
Assessment and treatment
But what symptoms should I really be concerned about? For any TBI that is associated with progressively declining neurological function or worsening headache, pupil asymmetry, seizures, intractable vomiting, ongoing disorientation or neurological deficit, slurred speech, or new bizarre behavior, you should immediately refer for emergency evaluation.
The good news is that the vast majority of mild TBI cases resolve without any intervention. It’s important for the physician to provide education and reassurance to the patient and family. Any interventions should be tailored to the specific symptoms while reinforcing good sleep hygiene, relaxation techniques, and limiting use of caffeine, tobacco, and alcohol. Return to normal functioning at work or school should be encouraged in a gradual, monitored fashion. Patients with a TBI who report ongoing symptoms need appropriate referral and a comprehensive treatment plan (Silver JM et al, Textbook of Traumatic Brain Injury, American Psychiatric Publishing, Inc; 2nd ed;2011).
Cognitive rehabilitation therapy (CRT)
You may have heard of cognitive rehabilitation therapy (CRT) as a treatment for TBI. But what exactly does it involve? And does it work? After a TBI there may be functional deficits that are both physical and mental in nature. CRT is a therapeutic process structured to improve the patient’s functioning in their daily lives. Patients are first guided through recognizing their strengths, weaknesses, and what deficits they want to improve. Then techniques are relearned when possible (solve the problem), or compensatory strategies are identified (work around the problem). The last step is to incorporate these relearned or new skills into daily life. This process can be applied to both physical and cognitive deficits that arise from a TBI.
CRT sessions should be tailored to the individual but most incorporate memory compensation techniques. Such techniques include having the patient write down at each session what was important to them, then reviewing their notes and memory of what was said during the next session. This method not only increases their participation in the therapy sessions but teaches them how to use the memory compensation techniques in their daily lives.
The evidence for CRT after stroke and moderate to severe TBI has long been established, showing improvement in the domains of memory, attention, and communication (Cicerone KD et al, Arch Phys Med Rehabil 2005;86(8):1681-1692). However, for mild TBI, CRT remains more controversial as there isn’t strong evidence for improved functional outcomes. The 2016 VA clinical guidelines recommend short-term CRT for moderate to severe TBI and discourages prolonged treatment courses without measurable improvements.
Sometimes the most concerning symptoms the patient will come to us for are the cognitive deficits and they may press for neuropsychological (NP) testing early. However, NP testing should not be done in the first 30 days. Most cognitive deficits of mild TBI will improve within this time period. And if the problems last longer than 30 days, NP testing may be helpful. Whenever referring for NP testing, be specific in why you are making the request. A targeted referral allows the NP examiner to choose the right tests to provide the most useful information.
Pharmacologic treatment
When considering medication treatment for symptoms following a TBI, there are several general guidelines to follow (Silver JM et al, Neurology 2006;67(5):748-755.2011). Again, most symptoms of a mild TBI will abate within a month, so watchful waiting and reassurance are important. Symptom improvement may continue throughout the first year as the brain continues to heal, so be sure to reassess the need for the medication intervention. Many times, the neuropsychiatric symptoms after a TBI can be complicated by concurrent major depressive disorder, PTSD, or a substance use disorder. Untreated depression can be the root cause of cognitive problems, irritability, sleep disturbance, fatigue, and headache. Be sure to perform a thorough psychiatric assessment so that you can tailor the treatment plan accordingly. Target specific symptoms or concurrent conditions with your medication choices. After a TBI the brain can be more susceptible to side effects of medications, underscoring the importance of “starting low, and going slow.”
Here are a few specific medication recommendations to target neuropsychiatric symptoms (Silver JM et al, 2011). For improving processing speed, methylphenidate has the most evidence. Donepezil and rivastigmine also may have some utility for treating memory impairment. When targeting depression and anxiety, SSRIs are first-line and choose a specific SSRI based on side effect profile and limiting medication interactions (sertraline, citalopram, and escitalopram are favorable choices) (Salter DL et al, J Head Trauma Rehabil 2016;31(4):E21-32). Be cautious with bupropion due to increased seizure risk. Caution is also advised with typical antipsychotics as they may inhibit neuronal recovery, and also benzodiazepines due to the memory impairment effects. For controlling mania or irritability, valproate is preferred due to its anti-seizure effect as well as having less cognitive side effects in long term treatment than other mood stabilizers (carbamazepine or lithium). Atypical antipsychotics may also be helpful in controlling irritability especially when combined with psychosis, and are preferred over typical antipsychotics. More recent research shows beneficial effects of amantadine in treating aggression from TBI even 6 months post-injury and more studies are evaluating its use in the acute phase after a severe TBI (Hammond FM et al, J Head Trauma Rehabil. 2017;32(5):308-318).
CATR Verdict: When treating patients with TBI, always remember that the brain has a great capacity for plasticity and recovery. Encourage patients to see their treatment as a process and journey. Take care to evaluate for comorbid mental health disorders, and handle accordingly. Those with substance use disorders, whether existing pre-TBI or newly occurring, should be encouraged to enter into treatment promptly. With the right combination of cognitive rehabilitation, pharmacotherapy, and a good therapeutic alliance, your patients can make great strides in recovery after a TBI.
Addiction TreatmentDefining TBI
Although there is no universally accepted definition for TBI, recently updated guidelines from the Department of Veterans Affairs (VA/DoD Clinical Practice Guideline for the Management of Concussion-mild Traumatic Brain Injury, 2016; https://tinyurl.com/y8e6owdx) state that a TBI is an injury to the brain caused by an external force accompanied by one of several clinical signs following the event). These signs can be an intracranial lesion, loss of consciousness, amnesia, confusion, slowed thinking, muscle weakness, sensory loss, or another neurological deficit. The severity of a TBI (mild, moderate, or severe) is determined by the symptoms immediately following the injury (see the VA TBI severity table below). If the patient meets different ratings for the different criteria, go with the more severe rating. The lay term “concussion” equates to a mild TBI. In addition to the neurological symptoms, patients may experience cognitive problems affecting their attention, memory, processing speed, and executive function. Mental health effects include irritability, impulsivity, depression, and anxiety. However, these symptoms can be an effect of the TBI or part of a comorbid, major depressive disorder, posttraumatic stress disorder (PTSD), or substance use disorder.
Table: Classification of TBI Severity
(Click to view full-size PDF.)
Assessment and treatment
But what symptoms should I really be concerned about? For any TBI that is associated with progressively declining neurological function or worsening headache, pupil asymmetry, seizures, intractable vomiting, ongoing disorientation or neurological deficit, slurred speech, or new bizarre behavior, you should immediately refer for emergency evaluation.
The good news is that the vast majority of mild TBI cases resolve without any intervention. It’s important for the physician to provide education and reassurance to the patient and family. Any interventions should be tailored to the specific symptoms while reinforcing good sleep hygiene, relaxation techniques, and limiting use of caffeine, tobacco, and alcohol. Return to normal functioning at work or school should be encouraged in a gradual, monitored fashion. Patients with a TBI who report ongoing symptoms need appropriate referral and a comprehensive treatment plan (Silver JM et al, Textbook of Traumatic Brain Injury, American Psychiatric Publishing, Inc; 2nd ed;2011).
Cognitive rehabilitation therapy (CRT)
You may have heard of cognitive rehabilitation therapy (CRT) as a treatment for TBI. But what exactly does it involve? And does it work? After a TBI there may be functional deficits that are both physical and mental in nature. CRT is a therapeutic process structured to improve the patient’s functioning in their daily lives. Patients are first guided through recognizing their strengths, weaknesses, and what deficits they want to improve. Then techniques are relearned when possible (solve the problem), or compensatory strategies are identified (work around the problem). The last step is to incorporate these relearned or new skills into daily life. This process can be applied to both physical and cognitive deficits that arise from a TBI.
CRT sessions should be tailored to the individual but most incorporate memory compensation techniques. Such techniques include having the patient write down at each session what was important to them, then reviewing their notes and memory of what was said during the next session. This method not only increases their participation in the therapy sessions but teaches them how to use the memory compensation techniques in their daily lives.
The evidence for CRT after stroke and moderate to severe TBI has long been established, showing improvement in the domains of memory, attention, and communication (Cicerone KD et al, Arch Phys Med Rehabil 2005;86(8):1681-1692). However, for mild TBI, CRT remains more controversial as there isn’t strong evidence for improved functional outcomes. The 2016 VA clinical guidelines recommend short-term CRT for moderate to severe TBI and discourages prolonged treatment courses without measurable improvements.
Sometimes the most concerning symptoms the patient will come to us for are the cognitive deficits and they may press for neuropsychological (NP) testing early. However, NP testing should not be done in the first 30 days. Most cognitive deficits of mild TBI will improve within this time period. And if the problems last longer than 30 days, NP testing may be helpful. Whenever referring for NP testing, be specific in why you are making the request. A targeted referral allows the NP examiner to choose the right tests to provide the most useful information.
Pharmacologic treatment
When considering medication treatment for symptoms following a TBI, there are several general guidelines to follow (Silver JM et al, Neurology 2006;67(5):748-755.2011). Again, most symptoms of a mild TBI will abate within a month, so watchful waiting and reassurance are important. Symptom improvement may continue throughout the first year as the brain continues to heal, so be sure to reassess the need for the medication intervention. Many times, the neuropsychiatric symptoms after a TBI can be complicated by concurrent major depressive disorder, PTSD, or a substance use disorder. Untreated depression can be the root cause of cognitive problems, irritability, sleep disturbance, fatigue, and headache. Be sure to perform a thorough psychiatric assessment so that you can tailor the treatment plan accordingly. Target specific symptoms or concurrent conditions with your medication choices. After a TBI the brain can be more susceptible to side effects of medications, underscoring the importance of “starting low, and going slow.”
Here are a few specific medication recommendations to target neuropsychiatric symptoms (Silver JM et al, 2011). For improving processing speed, methylphenidate has the most evidence. Donepezil and rivastigmine also may have some utility for treating memory impairment. When targeting depression and anxiety, SSRIs are first-line and choose a specific SSRI based on side effect profile and limiting medication interactions (sertraline, citalopram, and escitalopram are favorable choices) (Salter DL et al, J Head Trauma Rehabil 2016;31(4):E21-32). Be cautious with bupropion due to increased seizure risk. Caution is also advised with typical antipsychotics as they may inhibit neuronal recovery, and also benzodiazepines due to the memory impairment effects. For controlling mania or irritability, valproate is preferred due to its anti-seizure effect as well as having less cognitive side effects in long term treatment than other mood stabilizers (carbamazepine or lithium). Atypical antipsychotics may also be helpful in controlling irritability especially when combined with psychosis, and are preferred over typical antipsychotics. More recent research shows beneficial effects of amantadine in treating aggression from TBI even 6 months post-injury and more studies are evaluating its use in the acute phase after a severe TBI (Hammond FM et al, J Head Trauma Rehabil. 2017;32(5):308-318).
CATR Verdict: When treating patients with TBI, always remember that the brain has a great capacity for plasticity and recovery. Encourage patients to see their treatment as a process and journey. Take care to evaluate for comorbid mental health disorders, and handle accordingly. Those with substance use disorders, whether existing pre-TBI or newly occurring, should be encouraged to enter into treatment promptly. With the right combination of cognitive rehabilitation, pharmacotherapy, and a good therapeutic alliance, your patients can make great strides in recovery after a TBI.


Recommended


