
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
Screening and Prophylaxis of Infectious Diseases in Addiction Practice
 Sandra Springer, MD
Sandra Springer, MD
Associate Professor of Medicine in the Department of Internal Medicine, Yale School of Medicine. Director of the Infectious Disease Clinic (Newington) and Attending Infectious Disease Physician (West Haven), VA Connecticut Healthcare System.
Dr. Springer has disclosed that she has no relevant financial or other interests in any commercial companies pertaining to this educational activity.
CATR: Can you tell us about your background?
Dr. Springer: I’m an infectious disease doctor who is addiction medicine board certified as well. My background clinically is treating HIV and infectious diseases, as well as opioid use disorder (OUD) and alcohol use disorder (AUD). My research is about how to best integrate infectious disease and OUD treatments.
CATR: Should addiction practitioners pay attention to infectious disease screening and prophylaxis?
Dr. Springer: Yes, they should. The reason is that addiction providers treat a population that is at high risk of infectious diseases like hepatitis C (HCV) and HIV. They’re in a unique position to implement high-yield screening and prophylaxis measures, identify those who may not know they have an infectious disease, and then help them connect with treatment.
CATR: Why not just send people to their primary care physician or an infectious disease specialist?
Dr. Springer: The problem with that is most individuals don’t make that appointment. And it’s another barrier to care. For example, within the Veterans Affairs system, even though it’s the largest healthcare system in the country and has specialists, referrals to other clinics have been identified as a barrier. And it’s not just me saying it—the WHO, the CDC, and other groups like SAMHSA and HRSA encourage HCV and HIV screening and prevention in addiction settings.
CATR: That makes sense, but I can also see how psychiatrists might hesitate and think that the issue is outside of their area of expertise.
Dr. Springer: I get that a lot. And I hear the flip side from medicine saying, “Why should I screen for OUD or other substance use disorders (SUD)? Why should I treat OUD?” But we increasingly realize that a siloed approach is not ideal and in fact is harmful; and that basic measures can be provided in any setting, especially because the provider already has a relationship with the patient. And I’m not necessarily talking about treating HCV or HIV, but rather basic screening and preventive measures as well as referral to treatment, if needed. However, I do encourage general medicine doctors to provide medication treatment for OUD and AUD.
CATR: Let’s unpack this a bit. How do you screen for HIV?
Dr. Springer: The CDC recommends that all individuals ages 13–64 have at least 1 HIV test in their lifetime. And then you have additional HIV tests at least yearly or more often—for example, every 3 months if there are identified ongoing risk factors. Besides condomless sexual intercourse, a lot of people forget about injection drug use as a risk factor (www.cdc.gov/hiv/risk/idu.html; www.cdc.gov/hiv/guidelines/testing.html). There are rapid point-of-care tests for HIV screening that allow you to let people know within 15 minutes whether they may have HIV (www.tinyurl.com/y42guc7e). If the screen is positive, then you would order confirmatory blood testing called HIV p24 antigen/antibody test. Or you can do the HIV p24 antigen/antibody blood test initially, if you don’t have the rapid test. If the test is positive, then you refer the patient to an infectious disease specialist for treatment as well as obtain an HIV RNA viral load test for definitive confirmation.
CATR: And if it’s negative, then you counsel the patient about minimizing risk factors.
Dr. Springer: Yes, but if the test is negative, we would also recommend that you discuss whether the person qualifies for pre-exposure prophylaxis (PrEP) with Truvada or now Descovy—1 pill a day to prevent acquiring HIV—along with whatever addiction treatment you are providing. (For CDC guidelines for PrEP, see www.cdc.gov/hiv/pdf/risk/prep/cdc-hiv-prep-guidelines-2017.pdf. Also, see the “PrEP: Introduction to the Basics” article on page 5 for more information.)
CATR: Is written consent necessary for HIV testing?
Dr. Springer: No, there is no need for written consent. We call it opt-out HIV testing now, and it is the recommended way to offer testing. Typically, you tell the patient you are going to obtain an HIV test, and the patient then can opt out of testing. Counseling or written consent prior to testing was a barrier. If the HIV test is positive, you’ll want to counsel the patient and make sure there is adequate support, and if the test is negative, you’ll want to discuss harm reduction and PrEP. And you’ll also want to reassure the patient that, although there is no cure yet, HIV does not lower life expectancy with proper treatment.
CATR: What about HCV screening?
Dr. Springer: The CDC recommends that all baby boomers, who are people born between 1945 and 1965, be tested at least once, because HCV is more common in that age group. Otherwise, the recommendations include persons with past or current injection drug use. A full list of persons who should be offered HCV testing is provided on the CDC website (www.tinyurl.com/y3hdlgwf). There is a rapid screening test for HCV antibodies similar to HIV testing, which you’d follow by performing a confirmatory blood HCV antibody test. Again, you can do the blood HCV antibody if you don’t have the rapid one.
CATR: How do you interpret the results?
Dr. Springer: If the antibody test is negative, then the person doesn’t have HCV and never had HCV, and you have to provide a reminder that there is no vaccination for HCV. If the test is positive, then you want to get an HCV viral load. That’s because the HCV antibody does not indicate immunity or even active infection—it just means that the person had HCV at some point, even if it was fully treated. Most labs do a reflex viral load if the HCV antibody test is positive. And similarly, the idea behind screening is to identify active HCV and link patients to treatment. Current treatment is incredibly easy and curative—most regimens involve taking just 1 pill once a day for 8–12 weeks. Unfortunately, the HCV medications are very expensive; however, most Medicaid expansion states have now approved HCV medication treatment for any stage of HCV liver fibrosis. In fact, some methadone and buprenorphine clinics have successfully incorporated HCV treatment. (For up-to-date HCV treatment recommendations, please see www.hcvguidelines.org/treatment-naive.)
CATR: Since there is no vaccination for HIV or HCV, how frequently should we retest people with ongoing risk factors?
Dr. Springer: There is no standard recommendation. However, many of us recommend that, if people are partaking in high-risk behaviors, then they should be tested for HCV every 6 months, and as I mentioned before, every 3 months for HIV.
CATR: Could you walk us through screening for the other common types of hepatitis?
Dr. Springer: Hepatitis A (HAV) and B (HBV) infections are both preventable through vaccinations. HAV transmission is fecal/oral via contaminated food or water, so it’s not necessarily an infection you’d think of when you have a patient with a drug use history. However, people who use illicit drugs tend to have a higher risk of HAV infections. And it’s recommended that any person who uses illicit drugs, regardless of route, be screened and immunized for HAV. The test you want to get is the HAV IgG antibody. If the IgG is positive, then that means that the person has been vaccinated or had the disease. There is no chronic HAV. So, just document the presence of the antibody and the person is protected for life. If the IgG is negative, then you vaccinate the person or refer to primary care to receive the vaccination, and then you’re done. You don’t have to repeat the testing. (For the CDC’s recommendations related to HAV, see www.tinyurl.com/y2r62y96.)
CATR: And how do you go about HBV testing?
Dr. Springer: HBV is the most likely viral infection to be transmitted through sex and blood exposure, including through injection drug use, and it’s also preventable through vaccination. You should test and vaccinate for HBV anyone who is at risk through injection drug use or sexual transmission (www.tinyurl.com/y6yfdzbl). The recommendations are that you test for the HBV surface antibody and the HBV surface antigen.
CATR: Is interpreting HBV results more complicated than for HAV?
Dr. Springer: Yes, but not by a lot. There are 3 possibilities:
CATR: I recall there being a third antibody: c for core. Should we test for it too?
Dr. Springer: You can. A positive HBV core antibody test means that the person had an active infection at some point. I didn’t mention it, because I didn’t want to get too complicated. For a more complete approach to interpreting HBV results, readers can refer to an excellent table by the CDC at www.tinyurl.com/yawkn93m. And they can access a straightforward CDC algorithm for HAV, HBV, and HCV testing at www.tinyurl.com/y6xy3h9h.
CATR: Let’s switch gears a bit and talk about tuberculosis (TB) screening. Who should be screened?
Dr. Springer: People who have a history of injection drug use are considered at risk for having TB, as are people who have been incarcerated or are living in homeless shelters. And if you know that they have HIV, that’s another group that should be tested yearly for exposure to TB. I’d say these are the main risk factors to keep in mind in addiction practice. The CDC also has a good resource list for testing (see www.cdc.gov/tb/topic/testing/whobetested.htm). We used to do the tuberculin skin test, but now we’ve switched to the T-SPOT, which is a blood test. Some providers still use the tuberculin skin testing (PPD), but the problem is that patients often don’t come back to have the skin test read. T-SPOT is also more sensitive and specific. An important point to remember is that, if any of the tests for TB were EVER positive in the patient’s lifetime (PPD, T-SPOT, or other TB tests), the patient should NEVER be tested again. The result should be documented, and then an assessment for active disease should be documented. The documentation should also indicate whether the patient was referred for latent TB treatment or not.
CATR: Is this something the average outpatient addiction provider should be testing for?
Dr. Springer: Not necessarily, and there is no CDC recommendation that the addiction provider should be the one to do this. But it is recommended that residential programs test patients with risk factors—so, if you’re someone who works in a rehab or a long-term residential program, then you want to be familiar with this.
CATR: What should we do if the test is positive?
Dr. Springer: If it’s positive, you refer to an infectious disease doctor to monitor and provide treatment, if needed. And there’s no recommendation to have any contact precautions, unless the person has symptoms of active TB: fever, cough, night sweats, and weight loss. If the person has such symptoms and has a known history of untreated latent TB, or has risk factors for active TB and has never been tested, then the person should wear the appropriate mask and be transferred to have an assessment of etiology of symptoms and necessity for treatment in urgent care or an emergency room—the person can’t be out in the community with active TB, and treatment may need to be initiated in an isolated room. TB is the only infectious disease in the US for which there is legal enforcement for a patient to get hospitalized and treated.
CATR: Any additional advice for the busy clinician?
Dr. Springer: I hope people working in the addiction field are already on board with this, but I can’t overstress the importance of treating OUD with medications: buprenorphine, methadone, and extended release naltrexone. These are very effective medications that save lives, preserve health, and improve function. And they prevent contracting infectious diseases, especially those related to injection drug use: HIV, viral hepatitis, endocarditis, and cellulitis. Of course, we should also actively discuss harm reduction measures, such as clean needles and syringe exchange services. If you’re providing OUD and other SUD treatment, along with harm reduction strategies, and you’re paying attention to infectious disease issues, then you can be confident that you’re saving people’s lives and helping preserve their health.
CATR: Thank you for your time, Dr. Springer.
Addiction TreatmentDr. Springer: I’m an infectious disease doctor who is addiction medicine board certified as well. My background clinically is treating HIV and infectious diseases, as well as opioid use disorder (OUD) and alcohol use disorder (AUD). My research is about how to best integrate infectious disease and OUD treatments.
CATR: Should addiction practitioners pay attention to infectious disease screening and prophylaxis?
Dr. Springer: Yes, they should. The reason is that addiction providers treat a population that is at high risk of infectious diseases like hepatitis C (HCV) and HIV. They’re in a unique position to implement high-yield screening and prophylaxis measures, identify those who may not know they have an infectious disease, and then help them connect with treatment.
CATR: Why not just send people to their primary care physician or an infectious disease specialist?
Dr. Springer: The problem with that is most individuals don’t make that appointment. And it’s another barrier to care. For example, within the Veterans Affairs system, even though it’s the largest healthcare system in the country and has specialists, referrals to other clinics have been identified as a barrier. And it’s not just me saying it—the WHO, the CDC, and other groups like SAMHSA and HRSA encourage HCV and HIV screening and prevention in addiction settings.
CATR: That makes sense, but I can also see how psychiatrists might hesitate and think that the issue is outside of their area of expertise.
Dr. Springer: I get that a lot. And I hear the flip side from medicine saying, “Why should I screen for OUD or other substance use disorders (SUD)? Why should I treat OUD?” But we increasingly realize that a siloed approach is not ideal and in fact is harmful; and that basic measures can be provided in any setting, especially because the provider already has a relationship with the patient. And I’m not necessarily talking about treating HCV or HIV, but rather basic screening and preventive measures as well as referral to treatment, if needed. However, I do encourage general medicine doctors to provide medication treatment for OUD and AUD.
CATR: Let’s unpack this a bit. How do you screen for HIV?
Dr. Springer: The CDC recommends that all individuals ages 13–64 have at least 1 HIV test in their lifetime. And then you have additional HIV tests at least yearly or more often—for example, every 3 months if there are identified ongoing risk factors. Besides condomless sexual intercourse, a lot of people forget about injection drug use as a risk factor (www.cdc.gov/hiv/risk/idu.html; www.cdc.gov/hiv/guidelines/testing.html). There are rapid point-of-care tests for HIV screening that allow you to let people know within 15 minutes whether they may have HIV (www.tinyurl.com/y42guc7e). If the screen is positive, then you would order confirmatory blood testing called HIV p24 antigen/antibody test. Or you can do the HIV p24 antigen/antibody blood test initially, if you don’t have the rapid test. If the test is positive, then you refer the patient to an infectious disease specialist for treatment as well as obtain an HIV RNA viral load test for definitive confirmation.
CATR: And if it’s negative, then you counsel the patient about minimizing risk factors.
Dr. Springer: Yes, but if the test is negative, we would also recommend that you discuss whether the person qualifies for pre-exposure prophylaxis (PrEP) with Truvada or now Descovy—1 pill a day to prevent acquiring HIV—along with whatever addiction treatment you are providing. (For CDC guidelines for PrEP, see www.cdc.gov/hiv/pdf/risk/prep/cdc-hiv-prep-guidelines-2017.pdf. Also, see the “PrEP: Introduction to the Basics” article on page 5 for more information.)
CATR: Is written consent necessary for HIV testing?
Dr. Springer: No, there is no need for written consent. We call it opt-out HIV testing now, and it is the recommended way to offer testing. Typically, you tell the patient you are going to obtain an HIV test, and the patient then can opt out of testing. Counseling or written consent prior to testing was a barrier. If the HIV test is positive, you’ll want to counsel the patient and make sure there is adequate support, and if the test is negative, you’ll want to discuss harm reduction and PrEP. And you’ll also want to reassure the patient that, although there is no cure yet, HIV does not lower life expectancy with proper treatment.
CATR: What about HCV screening?
Dr. Springer: The CDC recommends that all baby boomers, who are people born between 1945 and 1965, be tested at least once, because HCV is more common in that age group. Otherwise, the recommendations include persons with past or current injection drug use. A full list of persons who should be offered HCV testing is provided on the CDC website (www.tinyurl.com/y3hdlgwf). There is a rapid screening test for HCV antibodies similar to HIV testing, which you’d follow by performing a confirmatory blood HCV antibody test. Again, you can do the blood HCV antibody if you don’t have the rapid one.
CATR: How do you interpret the results?
Dr. Springer: If the antibody test is negative, then the person doesn’t have HCV and never had HCV, and you have to provide a reminder that there is no vaccination for HCV. If the test is positive, then you want to get an HCV viral load. That’s because the HCV antibody does not indicate immunity or even active infection—it just means that the person had HCV at some point, even if it was fully treated. Most labs do a reflex viral load if the HCV antibody test is positive. And similarly, the idea behind screening is to identify active HCV and link patients to treatment. Current treatment is incredibly easy and curative—most regimens involve taking just 1 pill once a day for 8–12 weeks. Unfortunately, the HCV medications are very expensive; however, most Medicaid expansion states have now approved HCV medication treatment for any stage of HCV liver fibrosis. In fact, some methadone and buprenorphine clinics have successfully incorporated HCV treatment. (For up-to-date HCV treatment recommendations, please see www.hcvguidelines.org/treatment-naive.)
CATR: Since there is no vaccination for HIV or HCV, how frequently should we retest people with ongoing risk factors?
Dr. Springer: There is no standard recommendation. However, many of us recommend that, if people are partaking in high-risk behaviors, then they should be tested for HCV every 6 months, and as I mentioned before, every 3 months for HIV.
CATR: Could you walk us through screening for the other common types of hepatitis?
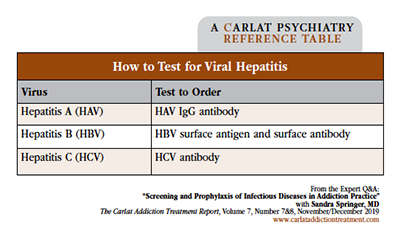
Dr. Springer: Hepatitis A (HAV) and B (HBV) infections are both preventable through vaccinations. HAV transmission is fecal/oral via contaminated food or water, so it’s not necessarily an infection you’d think of when you have a patient with a drug use history. However, people who use illicit drugs tend to have a higher risk of HAV infections. And it’s recommended that any person who uses illicit drugs, regardless of route, be screened and immunized for HAV. The test you want to get is the HAV IgG antibody. If the IgG is positive, then that means that the person has been vaccinated or had the disease. There is no chronic HAV. So, just document the presence of the antibody and the person is protected for life. If the IgG is negative, then you vaccinate the person or refer to primary care to receive the vaccination, and then you’re done. You don’t have to repeat the testing. (For the CDC’s recommendations related to HAV, see www.tinyurl.com/y2r62y96.)
CATR: And how do you go about HBV testing?
Dr. Springer: HBV is the most likely viral infection to be transmitted through sex and blood exposure, including through injection drug use, and it’s also preventable through vaccination. You should test and vaccinate for HBV anyone who is at risk through injection drug use or sexual transmission (www.tinyurl.com/y6yfdzbl). The recommendations are that you test for the HBV surface antibody and the HBV surface antigen.
CATR: Is interpreting HBV results more complicated than for HAV?
Dr. Springer: Yes, but not by a lot. There are 3 possibilities:
- If the HBV surface antibody is positive, then the person is immune and doesn’t need a vaccination or any further testing.
- If the surface antibody is negative and the surface antigen is negative, then the person has never been vaccinated and doesn’t have active infection, and the person should be vaccinated.
- If the surface antibody is negative and the surface antigen is positive, then the person has active infection, and you would refer the person to a liver or an infectious disease doctor and likely obtain an HBV viral load.
CATR: I recall there being a third antibody: c for core. Should we test for it too?
Dr. Springer: You can. A positive HBV core antibody test means that the person had an active infection at some point. I didn’t mention it, because I didn’t want to get too complicated. For a more complete approach to interpreting HBV results, readers can refer to an excellent table by the CDC at www.tinyurl.com/yawkn93m. And they can access a straightforward CDC algorithm for HAV, HBV, and HCV testing at www.tinyurl.com/y6xy3h9h.
Table: How to Test for Viral Hepatitis
Click to view full-size PDF.
CATR: Let’s switch gears a bit and talk about tuberculosis (TB) screening. Who should be screened?
Dr. Springer: People who have a history of injection drug use are considered at risk for having TB, as are people who have been incarcerated or are living in homeless shelters. And if you know that they have HIV, that’s another group that should be tested yearly for exposure to TB. I’d say these are the main risk factors to keep in mind in addiction practice. The CDC also has a good resource list for testing (see www.cdc.gov/tb/topic/testing/whobetested.htm). We used to do the tuberculin skin test, but now we’ve switched to the T-SPOT, which is a blood test. Some providers still use the tuberculin skin testing (PPD), but the problem is that patients often don’t come back to have the skin test read. T-SPOT is also more sensitive and specific. An important point to remember is that, if any of the tests for TB were EVER positive in the patient’s lifetime (PPD, T-SPOT, or other TB tests), the patient should NEVER be tested again. The result should be documented, and then an assessment for active disease should be documented. The documentation should also indicate whether the patient was referred for latent TB treatment or not.
CATR: Is this something the average outpatient addiction provider should be testing for?
Dr. Springer: Not necessarily, and there is no CDC recommendation that the addiction provider should be the one to do this. But it is recommended that residential programs test patients with risk factors—so, if you’re someone who works in a rehab or a long-term residential program, then you want to be familiar with this.
CATR: What should we do if the test is positive?
Dr. Springer: If it’s positive, you refer to an infectious disease doctor to monitor and provide treatment, if needed. And there’s no recommendation to have any contact precautions, unless the person has symptoms of active TB: fever, cough, night sweats, and weight loss. If the person has such symptoms and has a known history of untreated latent TB, or has risk factors for active TB and has never been tested, then the person should wear the appropriate mask and be transferred to have an assessment of etiology of symptoms and necessity for treatment in urgent care or an emergency room—the person can’t be out in the community with active TB, and treatment may need to be initiated in an isolated room. TB is the only infectious disease in the US for which there is legal enforcement for a patient to get hospitalized and treated.
CATR: Any additional advice for the busy clinician?
Dr. Springer: I hope people working in the addiction field are already on board with this, but I can’t overstress the importance of treating OUD with medications: buprenorphine, methadone, and extended release naltrexone. These are very effective medications that save lives, preserve health, and improve function. And they prevent contracting infectious diseases, especially those related to injection drug use: HIV, viral hepatitis, endocarditis, and cellulitis. Of course, we should also actively discuss harm reduction measures, such as clean needles and syringe exchange services. If you’re providing OUD and other SUD treatment, along with harm reduction strategies, and you’re paying attention to infectious disease issues, then you can be confident that you’re saving people’s lives and helping preserve their health.
CATR: Thank you for your time, Dr. Springer.



Recommended


