
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
Optimal Antidepressant Doses in Major Depression
Review of: Furukawa TA et al, Lancet Psychiatry;2019;6(7):601–609
Type of study: Systematic review and meta-analysis
Most antidepressants do not have a linear response curve. In other words, the benefits level off as the dose goes up. If the dose gets too high, the side effects start to outweigh those diminishing returns. What’s not clear is where the “sweet spot” lies for each antidepressant, and this study set out to capture that optimal dose range.
This dose-response meta-analysis included 77 double-blind, randomized, placebo-controlled trials of fixed-dose SSRIs (except fluvoxamine), venlafaxine, and mirtazapine in major depression (n = 19,365). Median trial length was 8 weeks (range = 4–12 weeks). Primary outcomes were efficacy (treatment response defined as 50% or greater reduction in depressive symptoms), tolerability (dropouts due to adverse effects), and acceptability (dropouts for any reason).
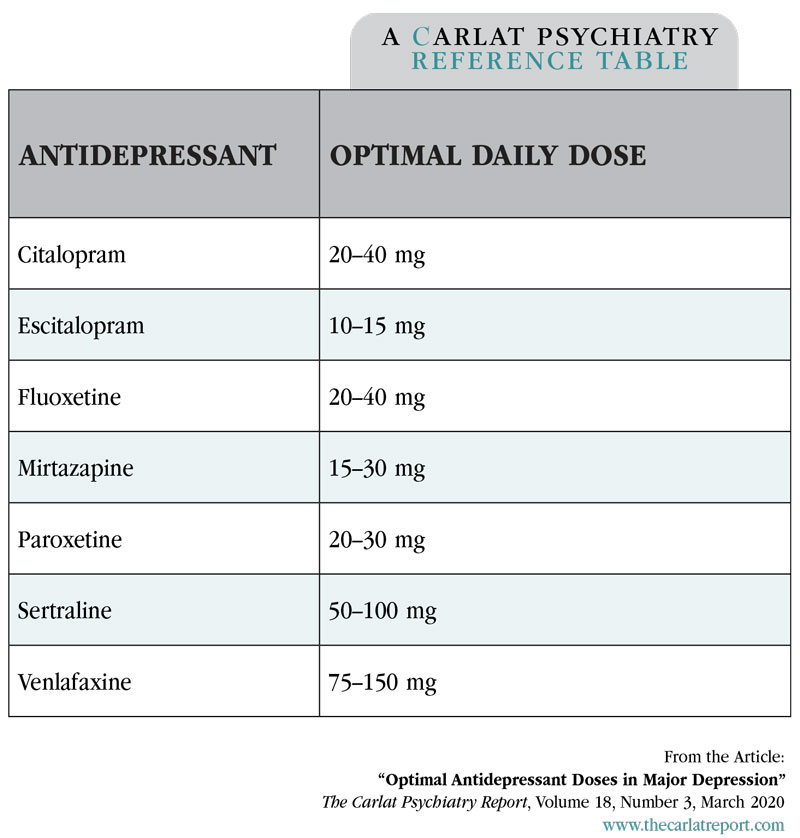
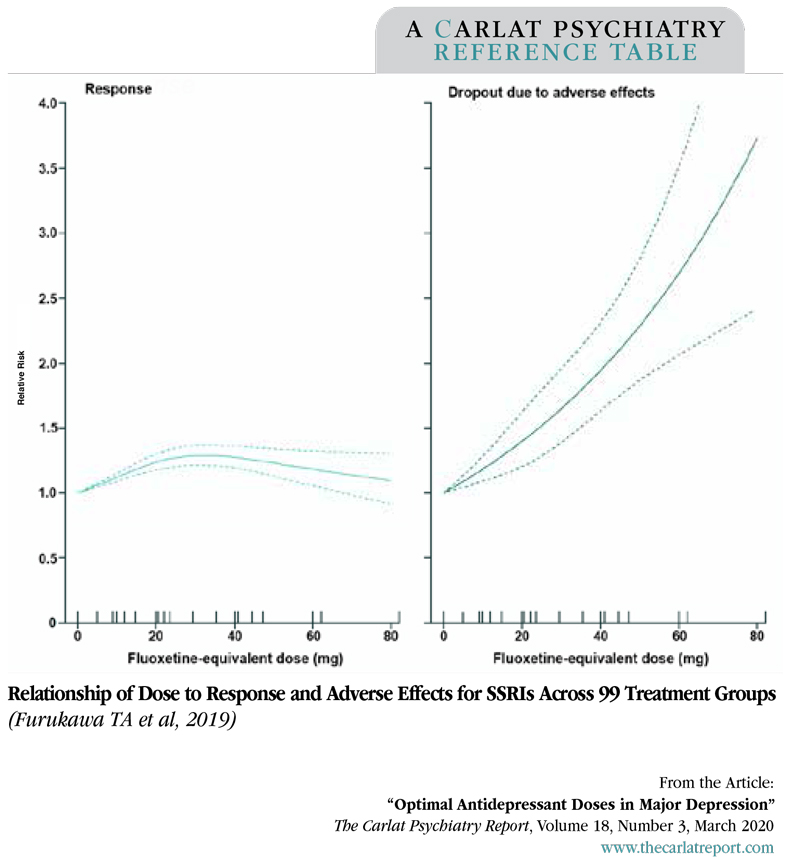
The best balance of efficacy, tolerability, and acceptability was achieved at low to medium doses of these antidepressants (see table). At higher doses (> 40 mg of fluoxetine equivalents), the benefits plateaued and dropouts from side effects showed steep, linear-to-exponential curves. Venlafaxine was unique in that its efficacy continued to increase up to 375 mg, though it started slowing at doses above 150 mg.
Table: Antidepressant Dosages
(Click to view full-size PDF.)
Graph: Relationship of Dose to Response and Adverse Effects for SSRIs Across 99 Treatment Groups
(Click to view full-size PDF.)
TCPR’s TAKE
When a patient does not recover fully on an antidepressant, it’s tempting to keep raising the dose. That strategy may work sometimes, but this study suggests that for many on second-generation antidepressants, an increased dose is more likely to cause side effects than therapeutic gains. If you go to a higher dose, measure the outcomes, and consider dropping back down if there’s no clear improvement.


Recommended


